Chow Ji-Jian, Leong Kevin M W, Shun-Shin Matthew, Jones Sian, Guttmann Oliver P, Mohiddin Saidi A, Lambiase Pier, Elliott Perry M, Ormerod Julian O M, Koa-Wing Michael, Lefroy David, Lim Phang Boon, Linton Nicholas W F, Ng Fu Siong, Qureshi Norman A, Whinnett Zachary I, Peters Nicholas S, Francis Darrel P, Varnava Amanda M, Kanagaratnam Prapa
National Heart and Lung Institute, Imperial College, London, United Kingdom.
Cardiology Department, Imperial College Healthcare NHS Trust, London, United Kingdom.
Front Physiol. 2024 Aug 14;15:1428709. doi: 10.3389/fphys.2024.1428709. eCollection 2024.
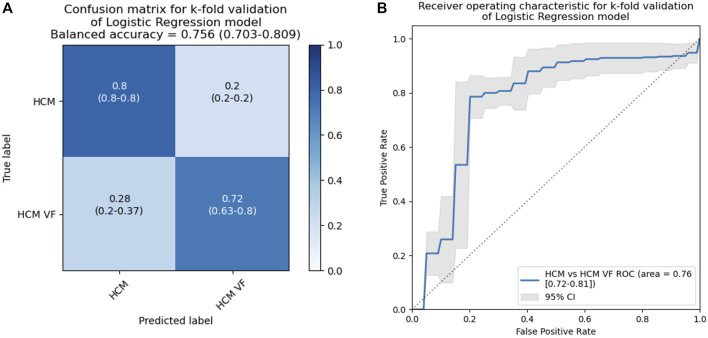
Patients with hypertrophic cardiomyopathy (HCM) are at risk for lethal ventricular arrhythmia, but the electrophysiological substrate behind this is not well-understood. We used non-invasive electrocardiographic imaging to characterize patients with HCM, including cardiac arrest survivors. HCM patients surviving ventricular fibrillation or hemodynamically unstable ventricular tachycardia (n = 17) were compared to HCM patients without a personal history of potentially lethal arrhythmia (n = 20) and a pooled control group with structurally normal hearts. Subjects underwent exercise testing by non-invasive electrocardiographic imaging to estimate epicardial electrophysiology. Visual inspection of reconstructed epicardial HCM maps revealed isolated patches of late activation time (AT), prolonged activation-recovery intervals (ARIs), as well as reversal of apico-basal trends in T-wave inversion and ARI compared to controls ( < 0.005 for all). AT and ARI were compared between groups. The pooled HCM group had longer mean AT (60.1 ms vs. 52.2 ms, < 0.001), activation dispersion (55.2 ms vs. 48.6 ms, = 0.026), and mean ARI (227 ms vs. 217 ms, = 0.016) than structurally normal heart controls. HCM ventricular arrhythmia survivors could be differentiated from HCM patients without a personal history of life-threatening arrhythmia by longer mean AT (63.2 ms vs. 57.4 ms, = 0.007), steeper activation gradients (0.45 ms/mm vs. 0.36 ms/mm, = 0.011), and longer mean ARI (234.0 ms vs. 221.4 ms, = 0.026). A logistic regression model including whole heart mean activation time and activation recovery interval could identify ventricular arrhythmia survivors from the HCM cohort, producing a C statistic of 0.76 (95% confidence interval 0.72-0.81), with an optimal sensitivity of 78.6% and a specificity of 79.8%. The HCM epicardial electrotype is characterized by delayed, dispersed conduction and prolonged, dispersed activation-recovery intervals. Combination of electrophysiologic measures with logistic regression can improve differentiation over single variables. Future studies could test such models prospectively for risk stratification of sudden death due to HCM.
肥厚型心肌病(HCM)患者存在发生致命性室性心律失常的风险,但其背后的电生理基质尚未完全明确。我们使用非侵入性心电图成像技术对HCM患者进行特征分析,包括心脏骤停幸存者。将发生心室颤动或血流动力学不稳定的室性心动过速的HCM患者(n = 17)与无潜在致命性心律失常个人史的HCM患者(n = 20)以及心脏结构正常的合并对照组进行比较。受试者通过非侵入性心电图成像进行运动试验,以评估心外膜电生理。对重建的心外膜HCM图进行视觉检查发现,与对照组相比,存在孤立的晚期激活时间(AT)区域、延长的激活-恢复间期(ARI),以及T波倒置和ARI的心尖-基底趋势反转(所有P均<0.005)。对各组之间的AT和ARI进行比较。与心脏结构正常的对照组相比,合并的HCM组平均AT更长(60.1毫秒对52.2毫秒,P<0.001)、激活离散度更大(55.2毫秒对48.6毫秒,P = 0.026)、平均ARI更长(227毫秒对217毫秒,P = 0.016)。与无危及生命心律失常个人史的HCM患者相比,HCM室性心律失常幸存者的平均AT更长(63.2毫秒对57.4毫秒,P = 0.007)、激活梯度更陡(0.45毫秒/毫米对0.36毫秒/毫米,P = 0.011)、平均ARI更长(234.0毫秒对221.4毫秒,P = 0.026)。一个包含全心平均激活时间和激活恢复间期的逻辑回归模型可以从HCM队列中识别出室性心律失常幸存者,C统计量为0.76(95%置信区间0.72 - 0.81),最佳敏感性为78.6%,特异性为79.8%。HCM心外膜电型的特征是传导延迟、离散,激活-恢复间期延长、离散。电生理测量与逻辑回归相结合可以比单一变量更好地进行区分。未来的研究可以前瞻性地测试此类模型用于HCM所致猝死的风险分层。