Department of Cardiac Surgery, First Affiliated Hospital of Sun Yat-sen University, Guangzhou, China.
Department of Epidemiology, Mailman School of Public Health, Columbia University, New York, NY, United States of America.
Ren Fail. 2024 Dec;46(2):2395450. doi: 10.1080/0886022X.2024.2395450. Epub 2024 Aug 30.
Patients on extracorporeal membrane oxygenation (ECMO) are often complex and have a high mortality rate. Currently, risk assessment and treatment decisions for patients receiving ECMO are controversial. Therefore, we sought to identify risk factors for mortality in patients receiving ECMO and provide a reference for patient management.
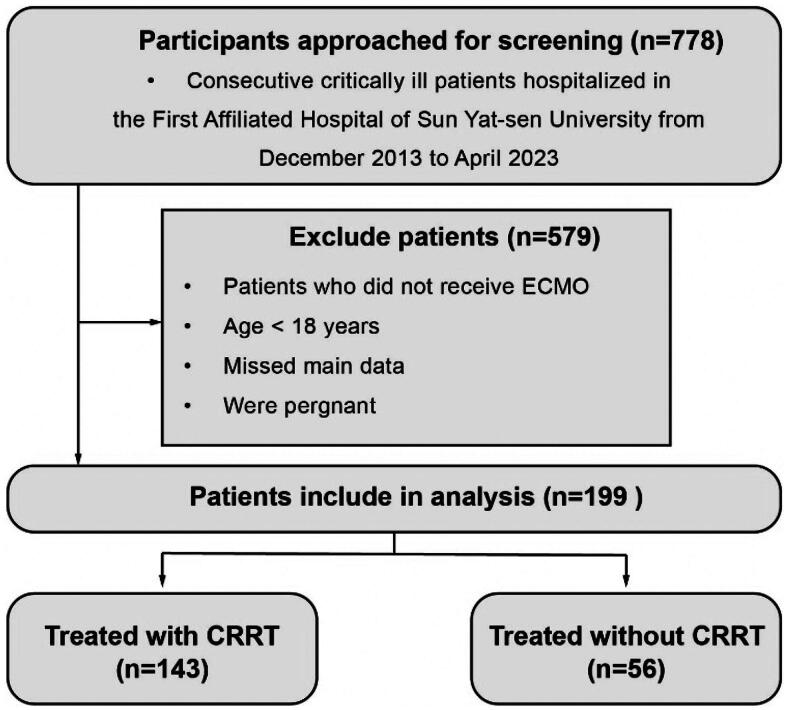
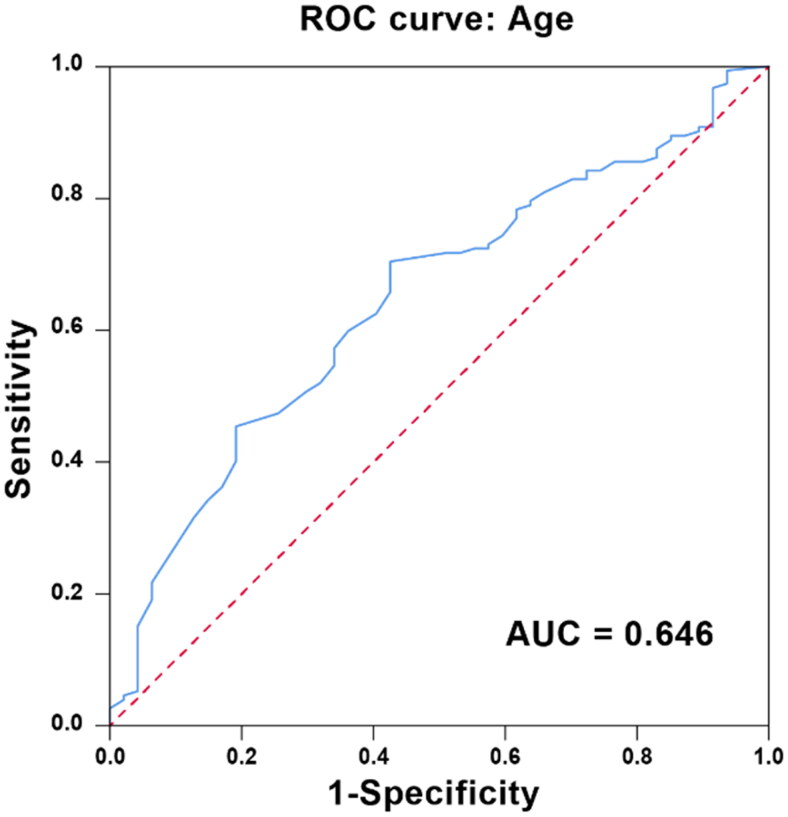
We retrospectively analyzed the clinical data of 199 patients who received ECMO support from December 2013 to April 2023. Univariate and multivariable logistic regression analyses were used to identify risk factors. The cutoff value was determined by receiver operating characteristic (ROC) curve analysis.
A total of 199 patients were selected for this study, and the mortality rate was 76.38%. More than half of the patients underwent surgery during hospitalization. Multivariable logistic regression analysis revealed that continuous renal replacement therapy (CRRT) implantation (OR = 2.994; 95% CI, 1.405-6.167; = 0.004) and age (OR = 1.021; 95% CI, 1.002-1.040; = 0.032) were the independent risk factors for mortality. In the ROC curve analysis, age had the best predictive effect (AUC 0.646, 95% CI 0.559-0.732, = 0.003) for death when the cutoff value was 48.5 years. Furthermore, in patients receiving combined CRRT and ECMO, lack of congenital heart disease and previous surgical history were the independent risk factors for mortality.
CRRT implantation and age were independent risk factors for patients with ECMO implantation in a predominantly surgical cohort. In patients receiving a combination of CRRT and ECMO, lack of congenital heart disease and previous surgical history were independent risk factors for mortality.
接受体外膜肺氧合(ECMO)治疗的患者通常病情复杂,死亡率较高。目前,对于接受 ECMO 治疗的患者的风险评估和治疗决策存在争议。因此,我们旨在确定接受 ECMO 治疗的患者死亡的风险因素,并为患者管理提供参考。
我们回顾性分析了 2013 年 12 月至 2023 年 4 月期间 199 例接受 ECMO 支持的患者的临床资料。采用单因素和多因素逻辑回归分析确定风险因素。通过接受者操作特征(ROC)曲线分析确定截断值。
本研究共纳入 199 例患者,死亡率为 76.38%。超过一半的患者在住院期间接受了手术。多因素逻辑回归分析显示,连续性肾脏替代治疗(CRRT)植入(OR=2.994;95%CI,1.405-6.167; = 0.004)和年龄(OR=1.021;95%CI,1.002-1.040; = 0.032)是死亡的独立危险因素。在 ROC 曲线分析中,年龄对死亡的预测效果最佳(AUC 0.646,95%CI 0.559-0.732, = 0.003),当截断值为 48.5 岁时。此外,在接受 CRRT 和 ECMO 联合治疗的患者中,无先天性心脏病和无既往手术史是死亡的独立危险因素。
在以手术为主的队列中,CRRT 植入和年龄是 ECMO 植入患者的独立危险因素。在接受 CRRT 和 ECMO 联合治疗的患者中,无先天性心脏病和无既往手术史是死亡的独立危险因素。