Bjerking Louise Hougesen, Skak-Hansen Kim Wadt, Heitmann Merete, Hove Jens Dahlgaard, Haahr-Pedersen Sune Ammentorp, Engblom Henrik, Erlinge David, Räder Sune Bernd Emil Werner, Brønnum-Schou Jens, Biering-Sørensen Tor, Kjærgaard Camilla Lyngby, Strange Søren, Galatius Søren, Prescott Eva Irene Bossano
Department of Cardiology, Copenhagen University Hospital-Bispebjerg and Frederiksberg, Bispebjerg Bakke 23, 2400 Copenhagen NV, Denmark.
Department of Cardiology, Copenhagen University Hospital-Amager and Hvidovre, Denmark.
Eur Heart J. 2025 Jan 7;46(2):117-128. doi: 10.1093/eurheartj/ehae570.
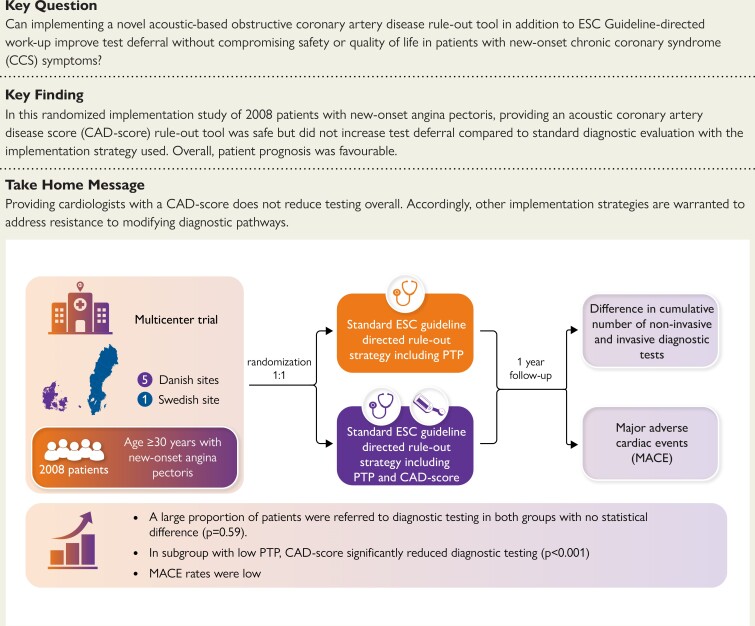
Overtesting of low-risk patients with suspect chronic coronary syndrome (CCS) is widespread. The acoustic-based coronary artery disease (CAD)-score has superior rule-out capabilities when added to pre-test probability (PTP). FILTER-SCAD tested whether providing a CAD-score and PTP to cardiologists was superior to PTP alone in limiting testing.
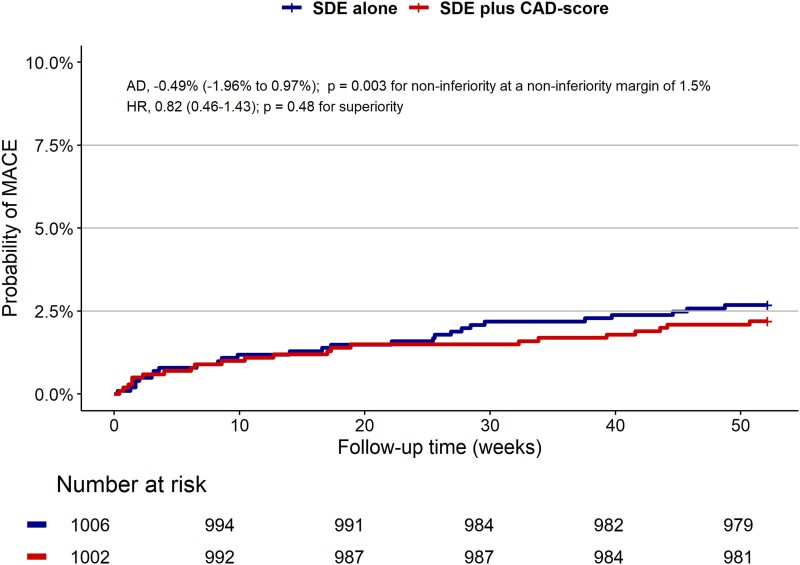
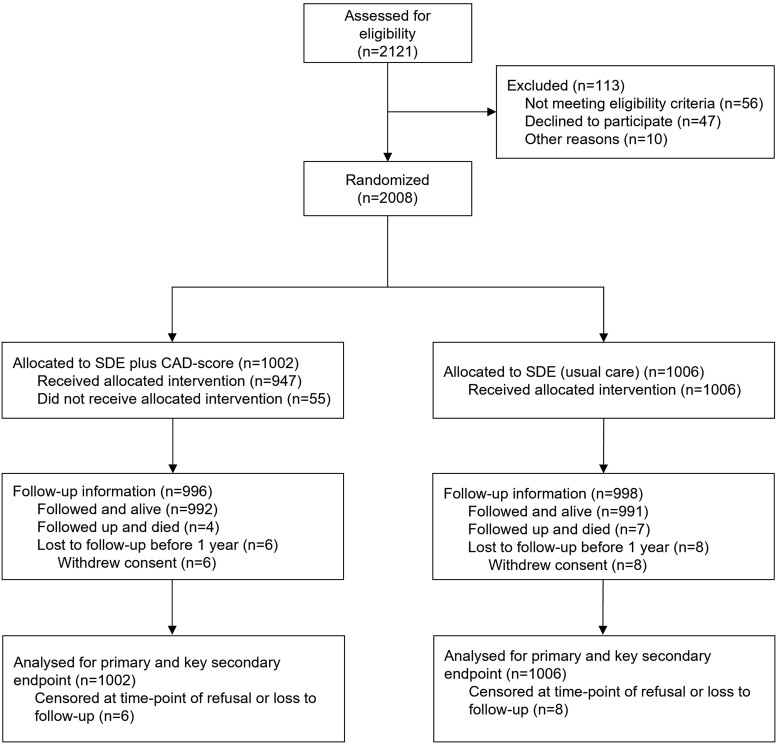
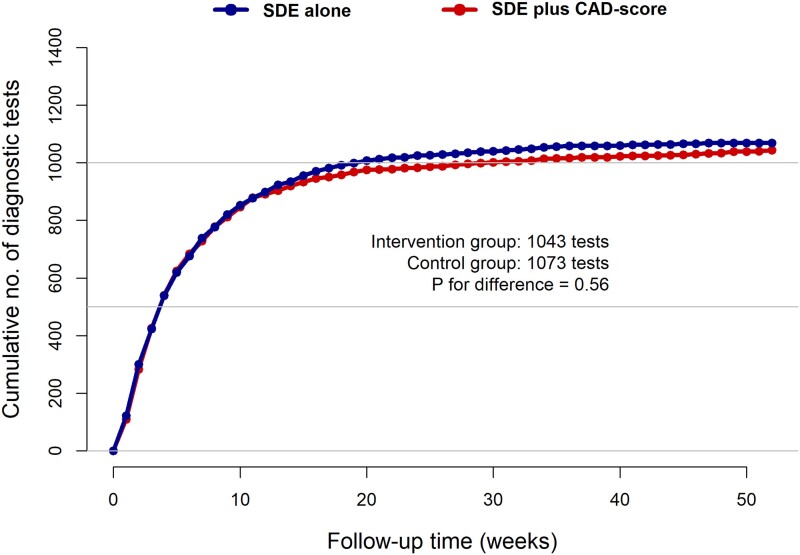
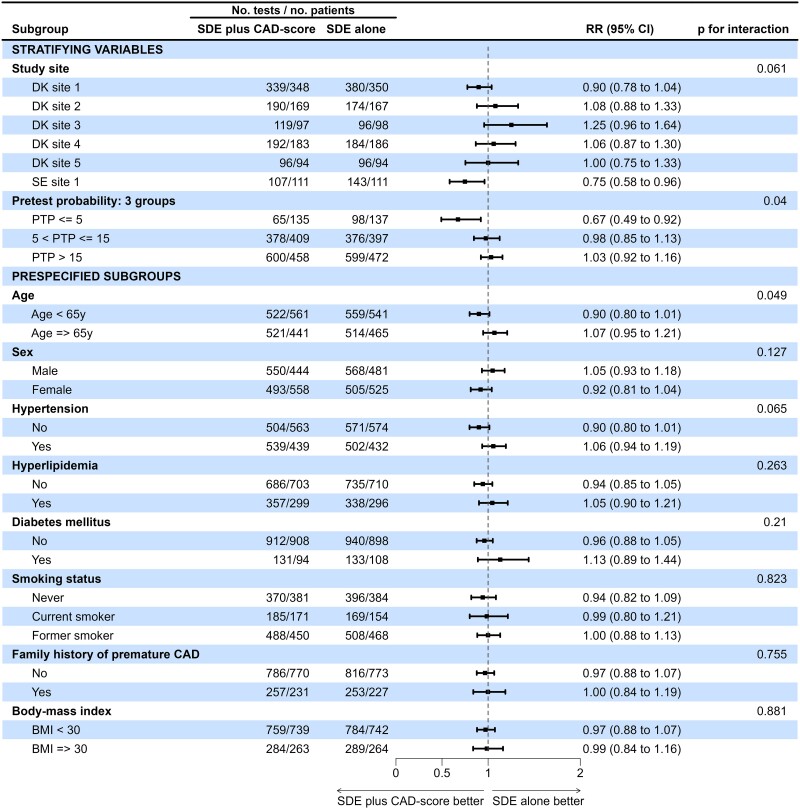
At six Danish and Swedish outpatient clinics, patients with suspected new-onset CCS were randomized to either standard diagnostic examination (SDE) with PTP, or SDE plus CAD-score, and cardiologists provided with corresponding recommended diagnostic flowcharts. The primary endpoint was cumulative number of diagnostic tests at one year and key safety endpoint major adverse cardiac events (MACE).
In total, 2008 patients (46% male, median age 63 years) were randomized from October 2019 to September 2022. When randomized to CAD-score (n = 1002), it was successfully measured in 94.5%. Overall, 13.5% had PTP ≤ 5%, and 39.5% had CAD-score ≤ 20. Testing was deferred in 22% with no differences in diagnostic tests between groups (P for superiority = .56). In the PTP ≤ 5% subgroup, the proportion with deferred testing increased from 28% to 52% (P < .001). Overall MACE was 2.4 per 100 person-years. Non-inferiority regarding safety was established, absolute risk difference 0.49% (95% confidence interval -1.96-0.97) (P for non-inferiority = .003). No differences were seen in angina-related health status or quality of life.
The implementation strategy of providing cardiologists with a CAD-score alongside SDE did not reduce testing overall but indicated a possible role in patients with low CCS likelihood. Further strategies are warranted to address resistance to modifying diagnostic pathways in this patient population.
对疑似慢性冠状动脉综合征(CCS)的低风险患者进行过度检查的情况普遍存在。基于声学的冠状动脉疾病(CAD)评分在加入预测试概率(PTP)时具有更好的排除能力。FILTER-SCAD研究旨在测试向心脏病专家提供CAD评分和PTP是否比单独提供PTP在限制检查方面更具优势。
在丹麦和瑞典的6家门诊诊所,将疑似新发CCS的患者随机分为接受仅提供PTP的标准诊断检查(SDE)组,或接受SDE加CAD评分组,同时为心脏病专家提供相应的推荐诊断流程图。主要终点是1年时诊断检查的累积数量,关键安全终点是主要不良心脏事件(MACE)。
2019年10月至2022年9月,共2008例患者(46%为男性,中位年龄63岁)被随机分组。随机分入CAD评分组(n = 1002)的患者中,94.5%成功进行了测量。总体而言,13.5%的患者PTP≤5%,39.5%的患者CAD评分≤20。22%的检查被推迟,两组间诊断检查无差异(优效性P = 0.56)。在PTP≤5%的亚组中,推迟检查的比例从28%增加到52%(P < 0.001)。总体MACE发生率为每100人年2.4例。确定了安全性方面的非劣效性,绝对风险差异为0.49%(95%置信区间 -1.96 - 0.97)(非劣效性P = 0.003)。在心绞痛相关健康状况或生活质量方面未发现差异。
在SDE的基础上向心脏病专家提供CAD评分的实施策略总体上并未减少检查,但表明在CCS可能性较低的患者中可能有作用。有必要采取进一步策略来解决该患者群体中对修改诊断途径的抵触情绪。