Division of Cardiac Surgery, Li Ka Shing Knowledge Institute of St Michael's Hospital, Unity Health Toronto, University of Toronto, Toronto, Ontario, Canada.
Baylor Scott and White Research Institute, Dallas, Texas, USA.
J Am Coll Cardiol. 2024 Oct 22;84(17):1603-1614. doi: 10.1016/j.jacc.2024.08.023. Epub 2024 Aug 30.
Obesity is a key factor in the development and progression of both heart failure with preserved ejection fraction (HFpEF) and atrial fibrillation (AF). In the STEP-HFpEF Program (comprising the STEP-HFpEF [Research Study to Investigate How Well Semaglutide Works in People Living With Heart Failure and Obesity] and STEP-HFpEF DM [Research Study to Look at How Well Semaglutide Works in People Living With Heart Failure, Obesity and Type 2 Diabetes] trials), once-weekly semaglutide 2.4 mg improved HF-related symptoms, physical limitations, and exercise function and reduced body weight in patients with obesity-related HFpEF. Whether the effects of semaglutide in this patient group differ in participants with and without AF (and across various AF types) has not been fully examined.
The goals of this study were: 1) to evaluate baseline characteristics and clinical features of patients with obesity-related HFpEF with and without a history of AF; and 2) to determine if the efficacy of semaglutide across all key trial outcomes are influenced by baseline history of AF (and AF types) in the STEP-HFpEF Program.
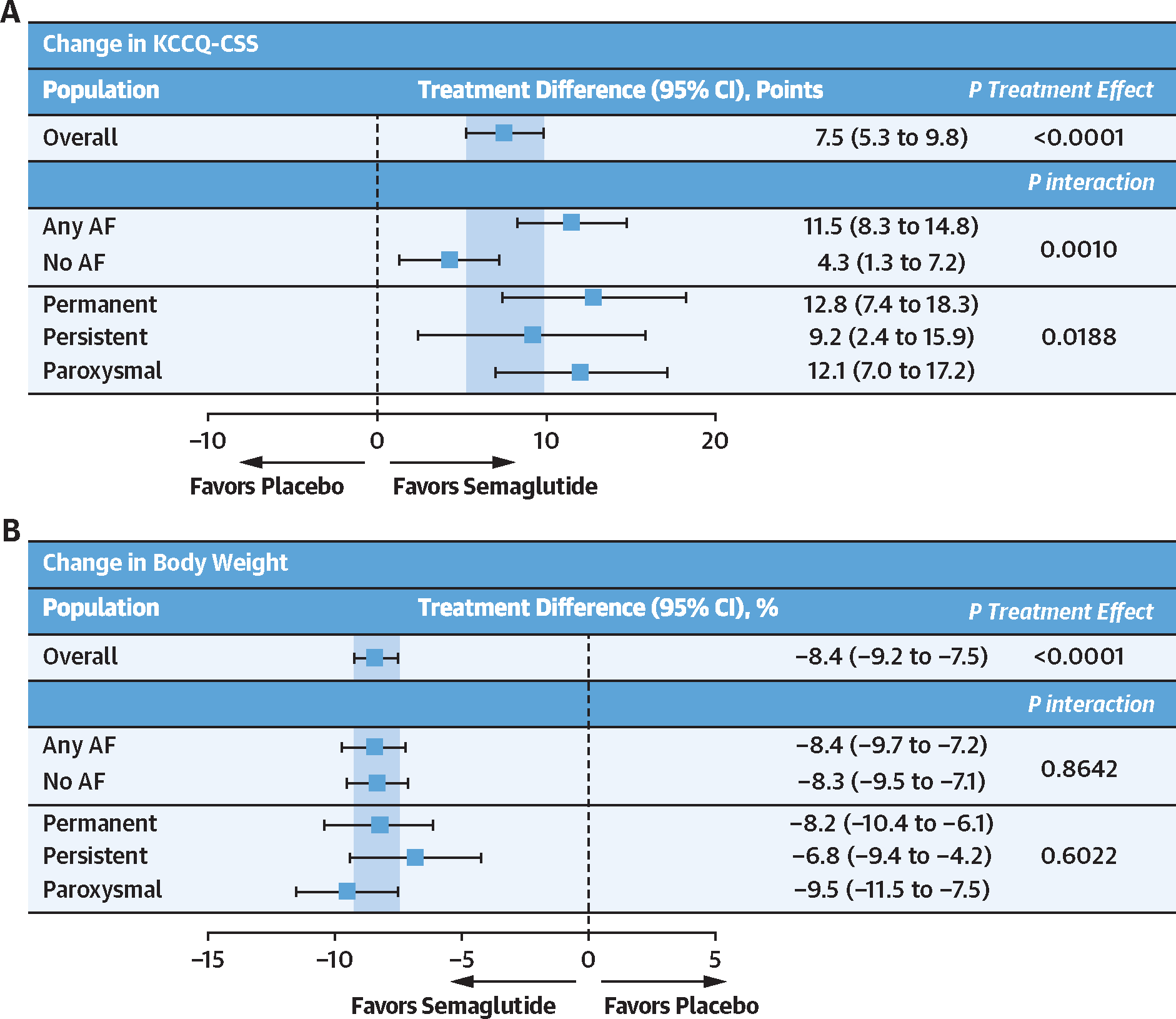
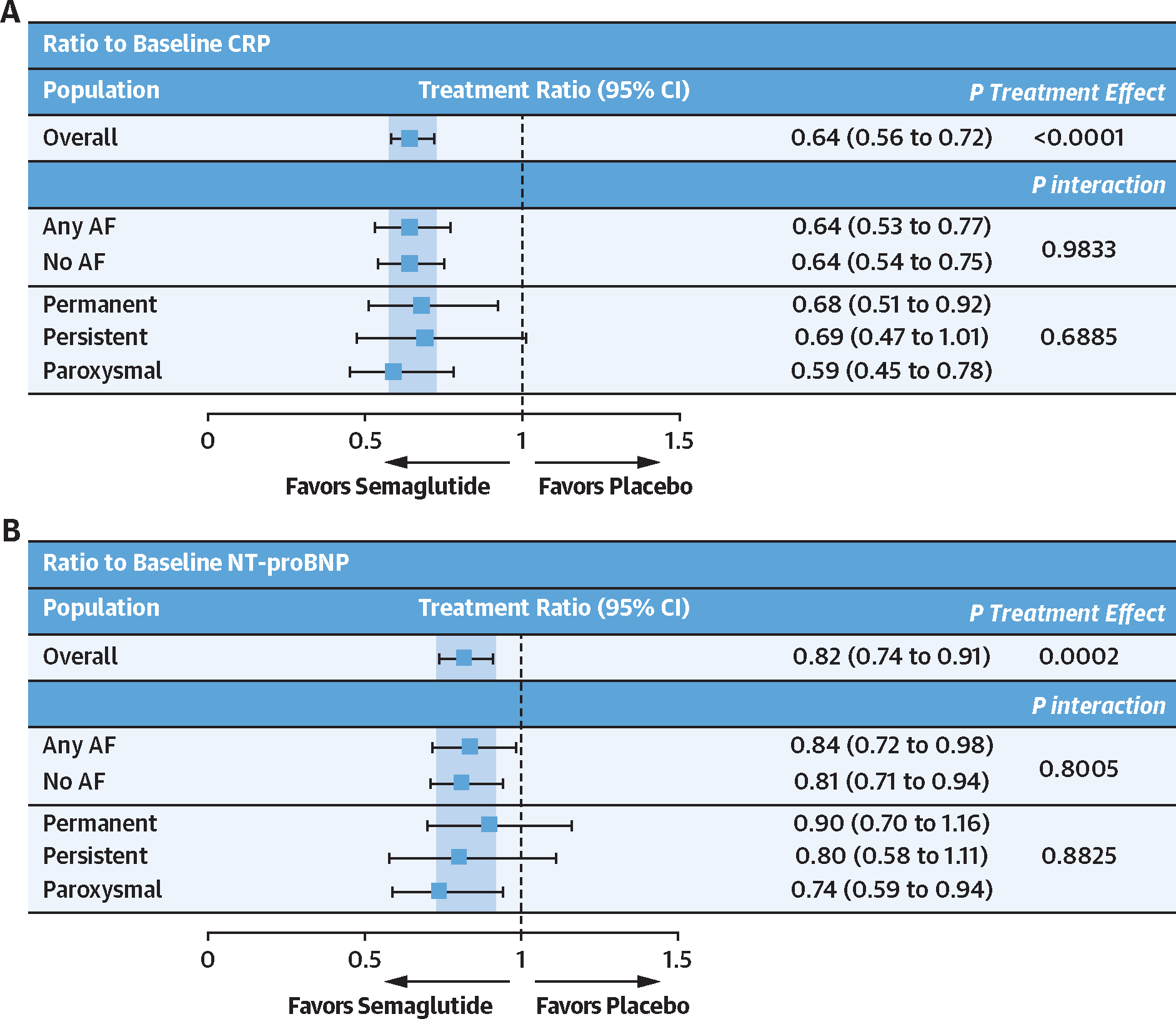
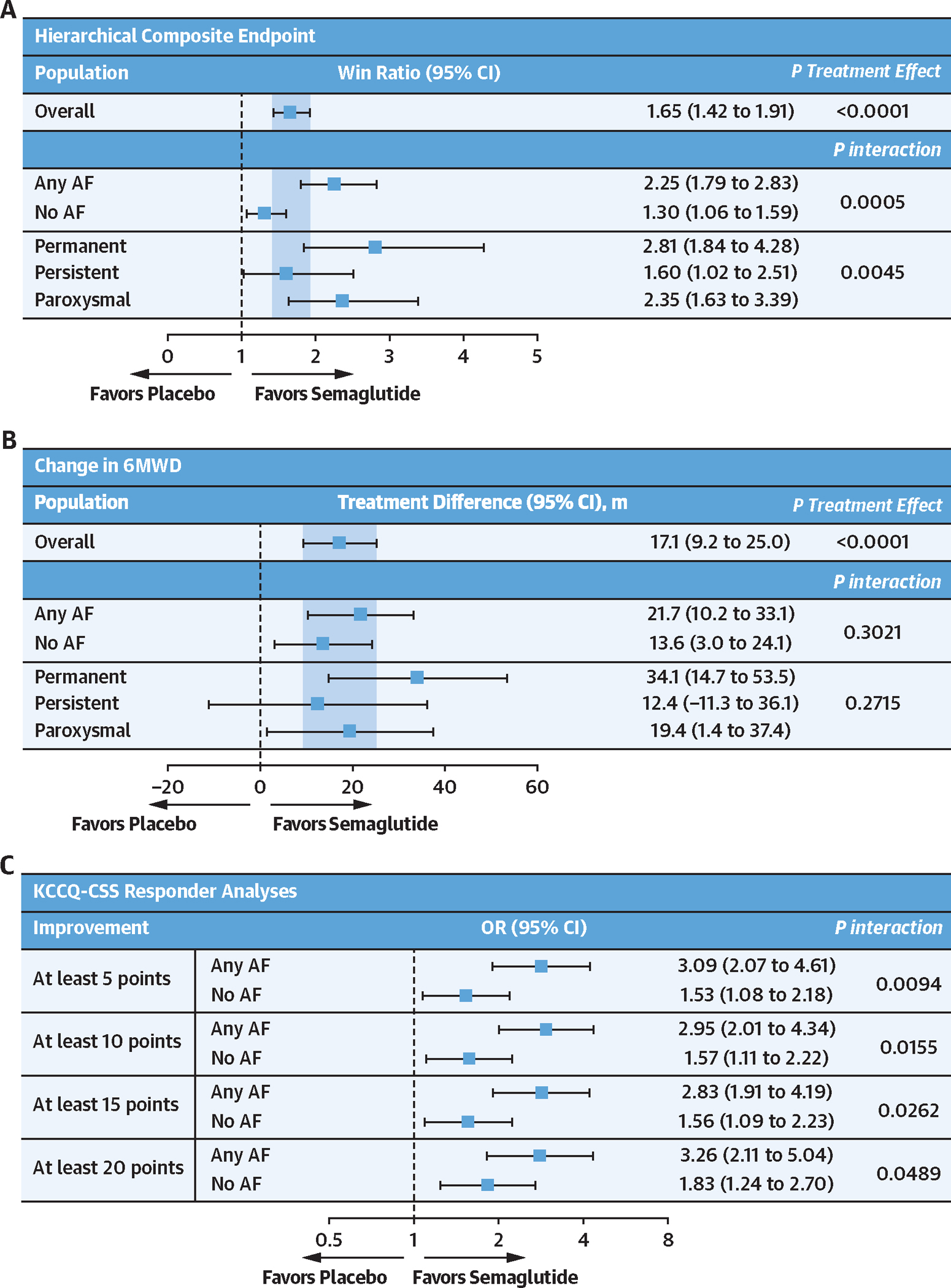
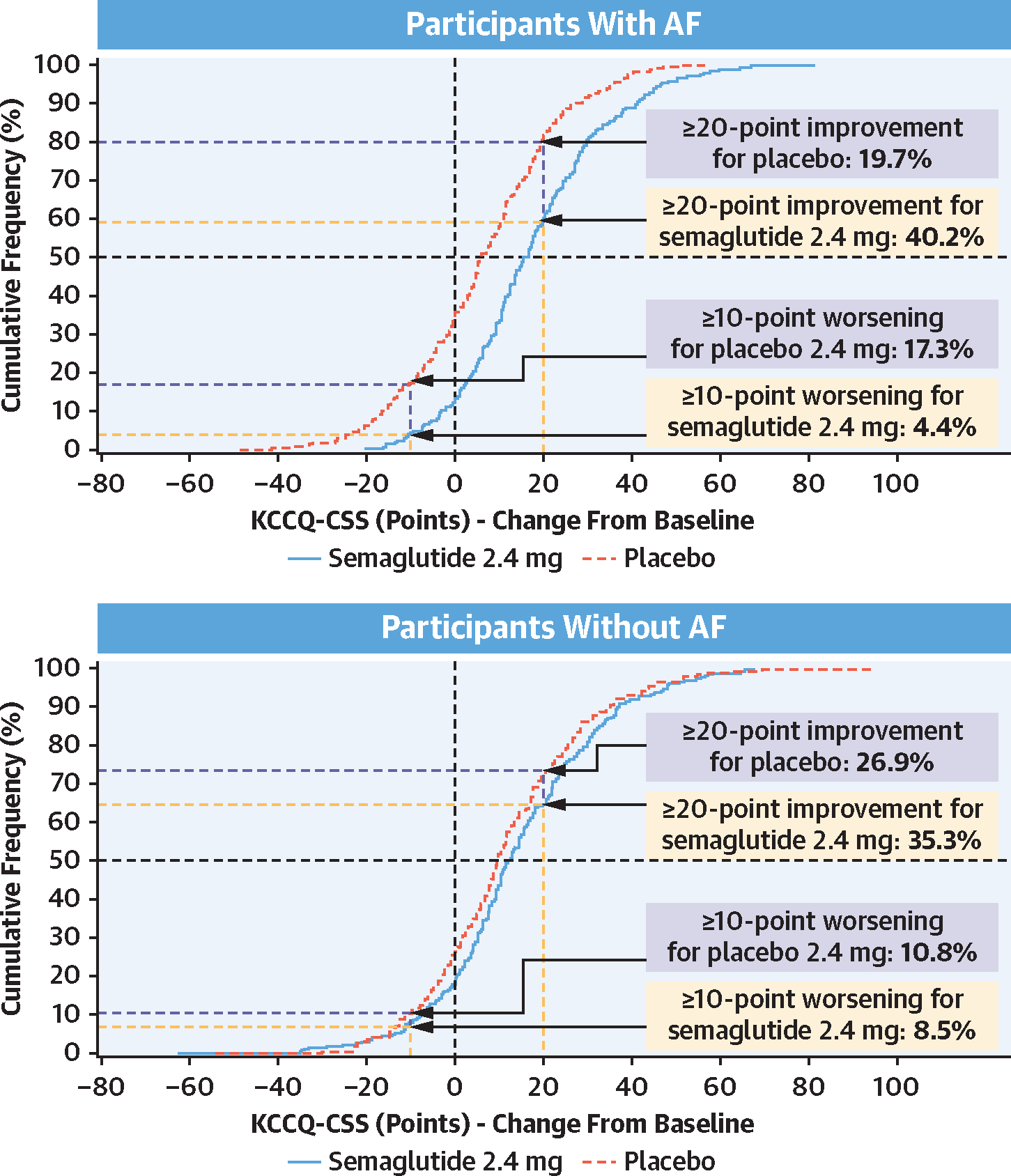
This was a secondary analysis of pooled data from the STEP-HFpEF and STEP-HFpEF DM trials. Patients with heart failure, left ventricular ejection fraction ≥45%, body mass index ≥30 kg/m, and Kansas City Cardiomyopathy Questionnaire-Clinical Summary Score (KCCQ-CSS) <90 points were randomized 1:1 to receive once-weekly semaglutide 2.4 mg or matching placebo for 52 weeks. Dual primary endpoints (change in KCCQ-CSS and percent change in body weight), confirmatory secondary endpoints (change in 6-minute walk distance; hierarchical composite endpoint comprising all-cause death, HF events, thresholds of change in KCCQ-CSS, and 6-minute walk distance; and C-reactive protein [CRP]), and exploratory endpoint (change in N-terminal pro-B-type natriuretic peptide [NT-proBNP]) were examined according to investigator-reported history of AF (yes/no). Responder analyses examined the proportions of patients who experienced a ≥5-, ≥10, ≥15, and ≥20-point improvement in KCCQ-CSS per history of AF.
Of the 1,145 participants, 518 (45%) had a history of AF (40% paroxysmal, 24% persistent AF, and 35% permanent AF) and 627 (55%) did not. Participants with (vs without) AF were older, more often male, had higher NT-proBNP levels, included a higher proportion of those with NYHA functional class III symptoms, and used more antithrombotic therapies, beta-blockers, and diuretics. Semaglutide led to larger improvements in KCCQ-CSS (11.5 points [95% CI: 8.3-14.8] vs 4.3 points [95% CI: 1.3-7.2]; P interaction = 0.001) and the hierarchal composite endpoint (win ratio of 2.25 [95% CI: 1.79-2.83] vs 1.30 [95% CI: 1.06-1.59]; P interaction < 0.001) in participants with AF vs without AF, respectively. The proportions of patients receiving semaglutide vs those receiving placebo experiencing ≥5-, ≥10-, ≥15-, and ≥20-point improvement in KCCQ-CSS were also higher in those with (vs without) AF (all P interaction values <0.05). Semaglutide consistently reduced CRP, NT-proBNP, and body weight regardless of AF status (all P interaction values not significant). There were fewer serious adverse events and serious cardiac disorders in participants treated with semaglutide vs placebo irrespective of AF history.
In the STEP-HFpEF Program, AF was observed in nearly one-half of patients with obesity-related HFpEF and was associated with several features of more advanced HF. Treatment with semaglutide led to significant improvements in HF-related symptoms, physical limitations, and exercise function, as well as reductions in weight, CRP, and NT-proBNP in people with and without AF and across AF types. The magnitude of semaglutide-mediated improvements in HF-related symptoms and physical limitations was more pronounced in those with AF vs without AF at baseline. (Research Study to Investigate How Well Semaglutide Works in People Living With Heart Failure and Obesity [STEP-HFpEF; NCT04788511]; Research Study to Look at How Well Semaglutide Works in People Living With Heart Failure, Obesity and Type 2 Diabetes [STEP-HFpEF DM; NCT04916470]).
肥胖是射血分数保留型心力衰竭(HFpEF)和心房颤动(AF)发展和进展的关键因素。在 STEP-HFpEF 计划(包括 STEP-HFpEF [研究 Semaglutide 在肥胖合并心力衰竭患者中的疗效] 和 STEP-HFpEF DM [研究 Semaglutide 在肥胖合并心力衰竭、2 型糖尿病患者中的疗效] 试验)中,每周一次的司美格鲁肽 2.4mg 可改善肥胖相关 HFpEF 患者的 HF 相关症状、身体限制和运动功能,并减轻体重。在肥胖相关 HFpEF 患者中,司美格鲁肽在有和没有 AF(以及各种 AF 类型)的患者中的疗效是否不同尚未完全研究。
本研究的目的是:1)评估肥胖相关 HFpEF 患者有和没有 AF 病史的基线特征和临床特征;2)确定司美格鲁肽在所有关键试验结局中的疗效是否受 STEP-HFpEF 计划中基线 AF 病史(和 AF 类型)的影响。
这是对 STEP-HFpEF 和 STEP-HFpEF DM 试验的汇总数据进行的二次分析。HF、左心室射血分数≥45%、BMI≥30kg/m2 和堪萨斯城心肌病问卷-临床综合评分(KCCQ-CSS)<90 分的心力衰竭患者按 1:1 随机接受每周一次司美格鲁肽 2.4mg 或匹配安慰剂治疗 52 周。双重主要终点(KCCQ-CSS 变化和体重百分比变化)、确认次要终点(6 分钟步行距离变化;包括全因死亡、HF 事件、KCCQ-CSS 变化阈值和 6 分钟步行距离变化的层次复合终点;和 C 反应蛋白 [CRP])和探索性终点(N 端脑利钠肽前体 [NT-proBNP] 变化)根据研究者报告的 AF 病史(是/否)进行检查。应答分析检查了根据 AF 病史(是/否),KCCQ-CSS 改善≥5、≥10、≥15 和≥20 点的患者比例。
在 1145 名参与者中,518 名(45%)有 AF 病史(40%阵发性,24%持续性 AF,35%永久性 AF),627 名(55%)没有。与无 AF 者相比,有 AF 者年龄较大,更常为男性,NT-proBNP 水平较高,NYHA 功能分级 III 症状比例较高,且更常使用抗血栓治疗、β受体阻滞剂和利尿剂。与无 AF 者相比,司美格鲁肽治疗可使 KCCQ-CSS(11.5 分[95%CI:8.3-14.8] vs 4.3 分[95%CI:1.3-7.2];P 交互<0.001)和层次复合终点(胜利比 2.25[95%CI:1.79-2.83] vs 1.30[95%CI:1.06-1.59];P 交互<0.001)显著改善,分别。与无 AF 者相比,有 AF 者接受司美格鲁肽治疗与安慰剂治疗的患者中,KCCQ-CSS 改善≥5、≥10、≥15 和≥20 点的比例也更高(所有 P 交互值均<0.05)。无论 AF 状态如何,司美格鲁肽均能持续降低 CRP、NT-proBNP 和体重(所有 P 值交互均无显著意义)。与安慰剂组相比,接受司美格鲁肽治疗的患者中严重不良事件和严重心脏疾病的发生率较低,无论 AF 病史如何。
在 STEP-HFpEF 计划中,近一半肥胖相关 HFpEF 患者存在 AF,且与更晚期 HF 的多个特征有关。在有和没有 AF 以及各种 AF 类型的患者中,司美格鲁肽治疗可显著改善 HF 相关症状、身体限制和运动功能,降低体重、CRP 和 NT-proBNP。与无 AF 患者相比,基线时 AF 患者的 HF 相关症状和身体限制改善幅度更大。(研究 Semaglutide 在肥胖合并心力衰竭患者中的疗效[STEP-HFpEF;NCT04788511];研究 Semaglutide 在肥胖合并心力衰竭、2 型糖尿病患者中的疗效[STEP-HFpEF DM;NCT04916470])。