Vascular Medicine Outcomes (VAMOS) Program, Section of Cardiovascular Medicine, Yale University, New Haven, CT, USA.
Department of Psychiatry, Yale School of Medicine, New Haven, CT, USA.
Vasc Med. 2024 Oct;29(5):496-506. doi: 10.1177/1358863X241268727. Epub 2024 Sep 1.
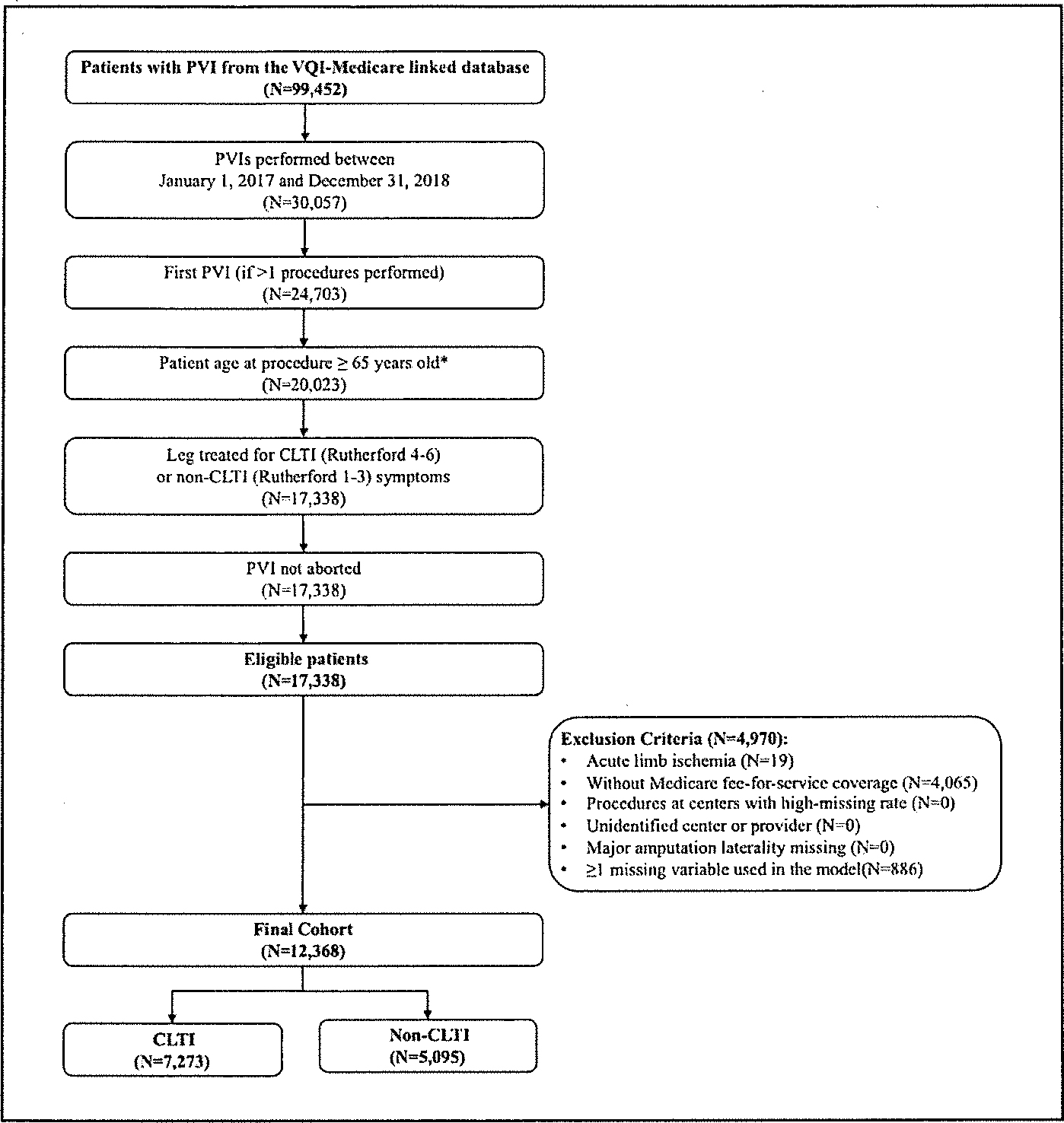
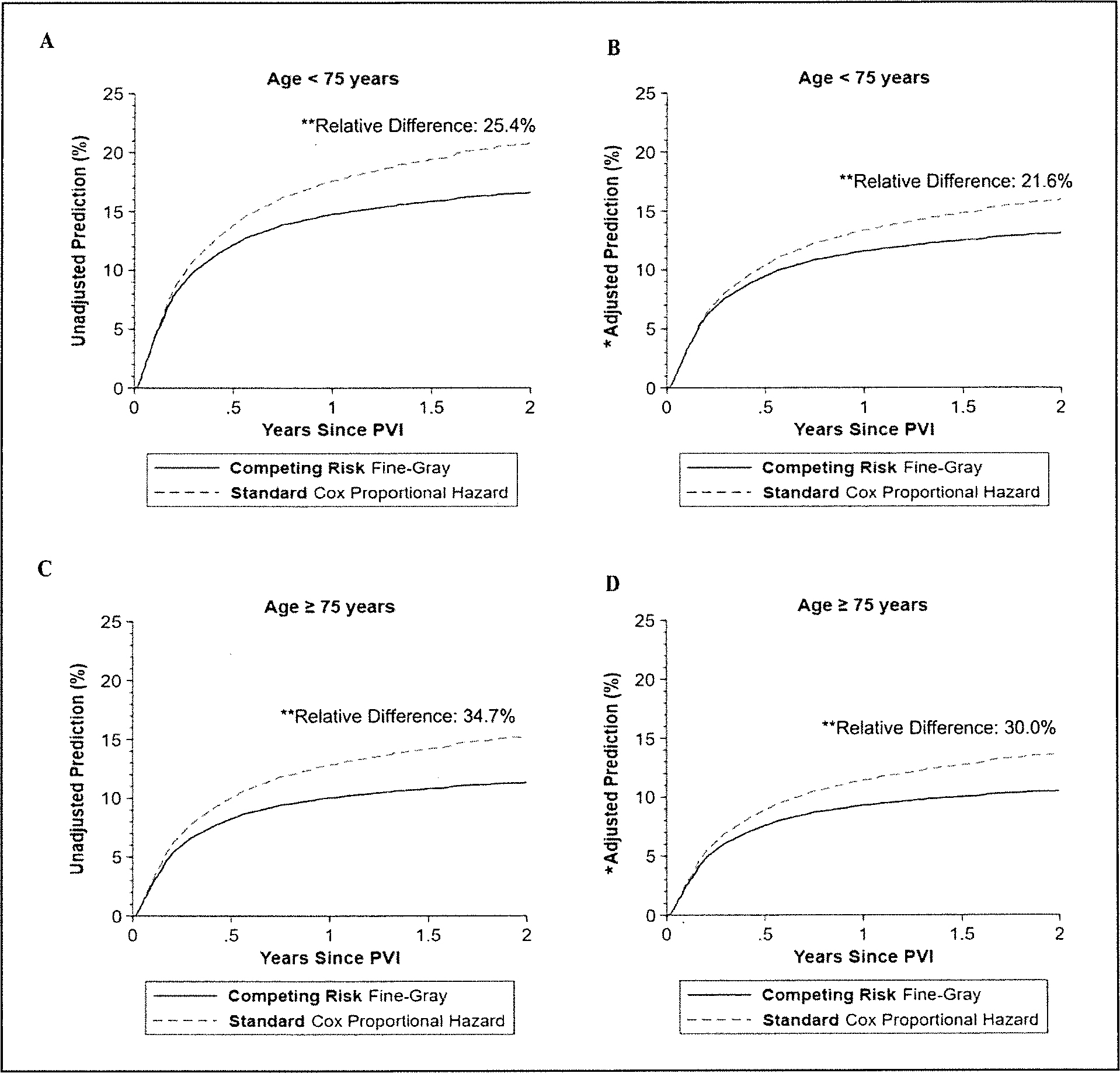
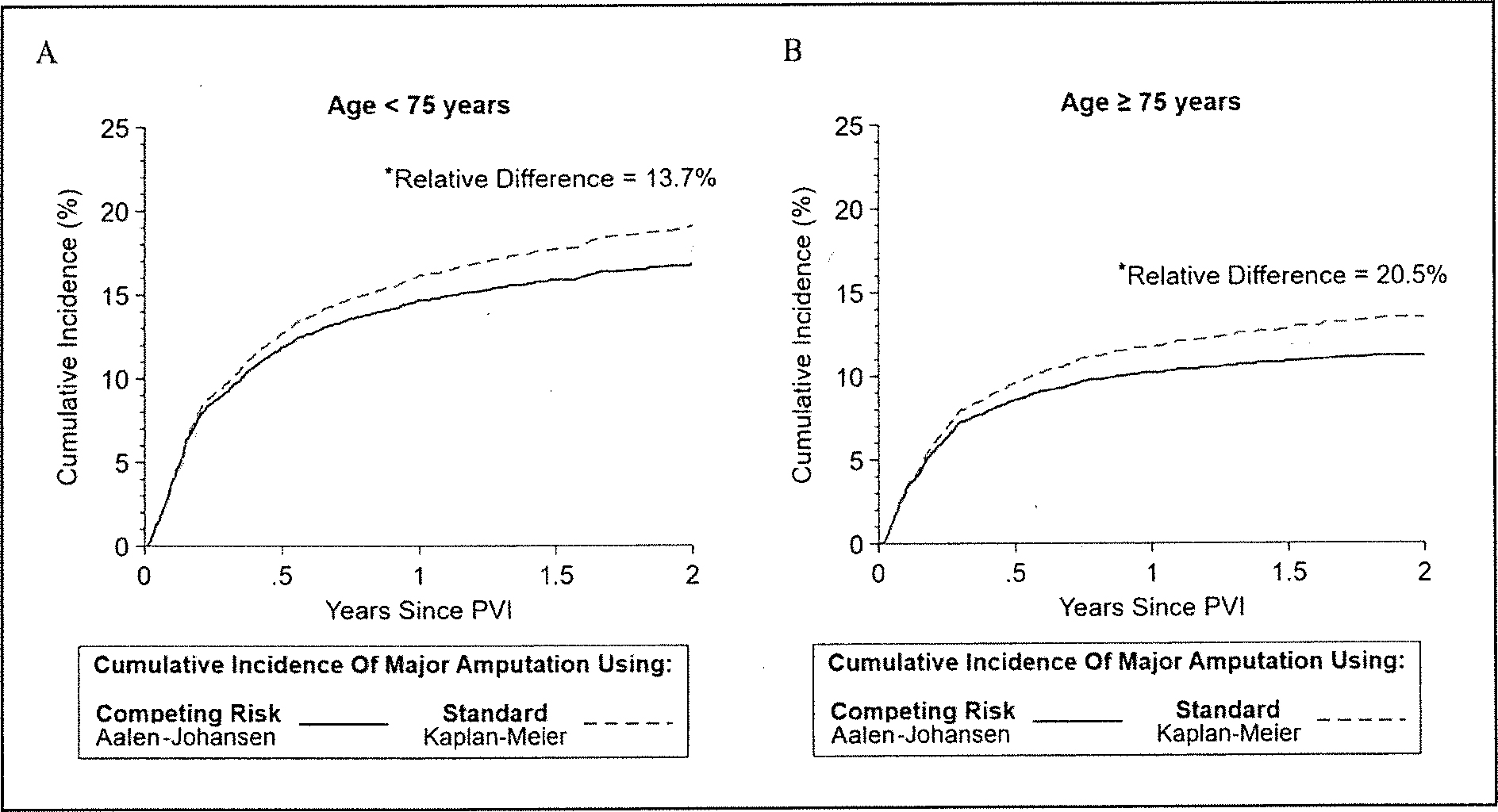
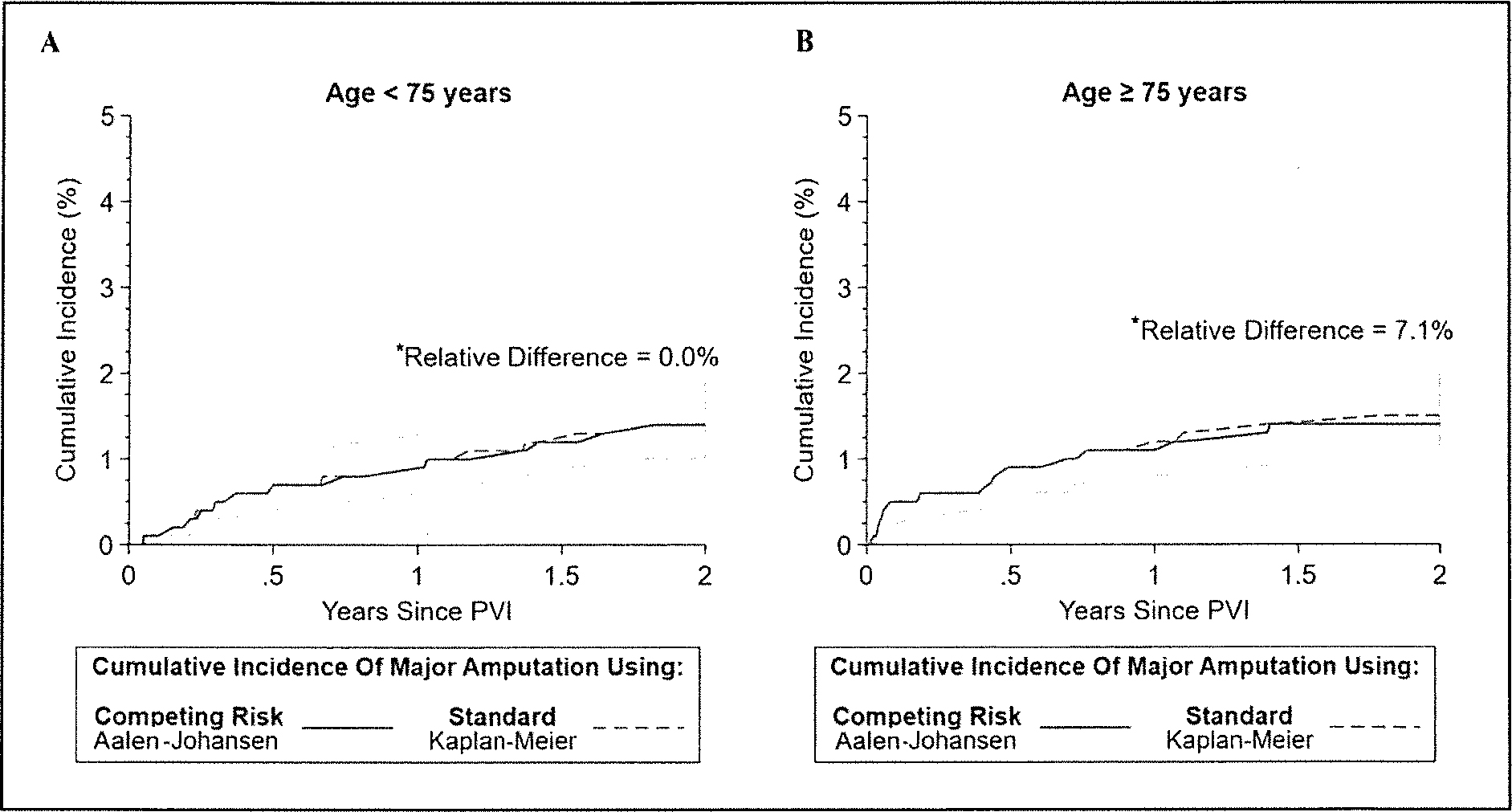
Patients with peripheral artery disease face high amputation and mortality risk. When assessing vascular outcomes, consideration of mortality as a competing risk is not routine. We hypothesize standard time-to-event methods will overestimate major amputation risk in chronic limb-threatening ischemia (CLTI) and non-CLTI. : Patients undergoing peripheral vascular intervention from 2017 to 2018 were abstracted from the Vascular Quality Initiative registry and stratified by mean age (⩾ 75 vs < 75 years). Mortality and amputation data were obtained from Medicare claims. The 2-year cumulative incidence function (CIF) and risk of major amputation from standard time-to-event analysis (1 - Kaplan-Meier and Cox regression) were compared with competing risk analysis (Aalen-Johansen and Fine-Gray model) in CLTI and non-CLTI. : A total of 7273 patients with CLTI and 5095 with non-CLTI were included. At 2-year follow up, 13.1% of patients underwent major amputation and 33.4% died without major amputation in the CLTI cohort; 1.3% and 10.7%, respectively, in the non-CLTI cohort. In CLTI, standard time-to-event analysis overestimated the 2-year CIF of major amputation by 20.5% and 13.7%, respectively, in patients ⩾ 75 and < 75 years old compared with competing risk analysis. The standard Cox regression overestimated adjusted 2-year major amputation risk in patients ⩾ 75 versus < 75 years old by 7.0%. In non-CLTI, the CIF was overestimated by 7.1% in patients ⩾ 75 years, and the adjusted risk was overestimated by 5.1% compared with competing risk analysis. : Standard time-to-event analysis overestimates the incidence and risk of major amputation, especially in CLTI. Competing risk analyses are alternative approaches to estimate accurately amputation risk in vascular outcomes research.
患有外周动脉疾病的患者面临高截肢和死亡率风险。在评估血管结果时,并不常规考虑死亡率作为竞争风险。我们假设标准时间事件方法将高估慢性肢体威胁性缺血 (CLTI) 和非 CLTI 的主要截肢风险。
从血管质量倡议登记处提取 2017 年至 2018 年接受外周血管介入治疗的患者,并按平均年龄(⩾ 75 岁与 < 75 岁)分层。从医疗保险索赔中获得死亡率和截肢数据。在 CLTI 和非 CLTI 中,比较标准时间事件分析(1 - Kaplan-Meier 和 Cox 回归)的主要截肢 2 年累积发生率函数(CIF)和风险与竞争风险分析(Aalen-Johansen 和 Fine-Gray 模型)。
共纳入 7273 例 CLTI 患者和 5095 例非 CLTI 患者。在 2 年随访中,CLTI 队列中有 13.1%的患者接受了主要截肢,33.4%的患者在没有主要截肢的情况下死亡;非 CLTI 队列中分别为 1.3%和 10.7%。在 CLTI 中,标准时间事件分析高估了 2 年主要截肢 CIF,分别为年龄 ⩾ 75 岁和 < 75 岁的患者高估了 20.5%和 13.7%。标准 Cox 回归高估了年龄 ⩾ 75 岁与 < 75 岁的患者 2 年主要截肢风险调整后 7.0%。在非 CLTI 中,年龄 ⩾ 75 岁的患者 CIF 高估了 7.1%,与竞争风险分析相比,调整后的风险高估了 5.1%。
标准时间事件分析高估了主要截肢的发生率和风险,尤其是在 CLTI 中。竞争风险分析是一种估计血管结局研究中截肢风险的替代方法。