The Kirby Institute, University of New South Wales, Sydney, Australia.
The Papua New Guinea Institute of Medical Research, Goroka, Papua New Guinea.
Int J Equity Health. 2024 Sep 2;23(1):176. doi: 10.1186/s12939-024-02241-0.
Although global poverty rates have declined in the last decade, the fall in the Asia-Pacific region has been slow relative to the rest of the world. Poverty continues to be a major cause of poor maternal and newborn health, and a barrier to accessing timely antenatal care. Papua New Guinea has one of the highest poverty rates and some of the worst maternal and neonatal outcomes in the Asia-Pacific region. Few studies have investigated equity in antenatal care utilization in this setting. We explored equity in antenatal care utilization and the determinants of service utilization, which include a measure of multidimensional poverty in Papua New Guinea.
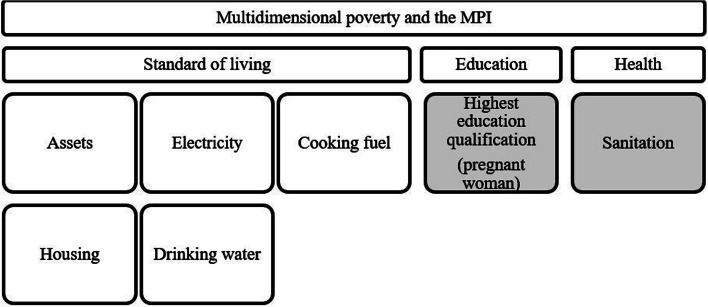
To explore the association between poverty and antenatal care utilization this study uses data from a ten-cluster randomized controlled trial. The poverty headcount, average poverty gap, adjusted poverty headcount, and multidimensional poverty index of antenatal clinic attendees are derived using the Alkire-Foster method. The distribution of service utilization is explored using the multidimensional poverty index, followed by multivariate regression analyses to evaluate the determinants of service utilization.
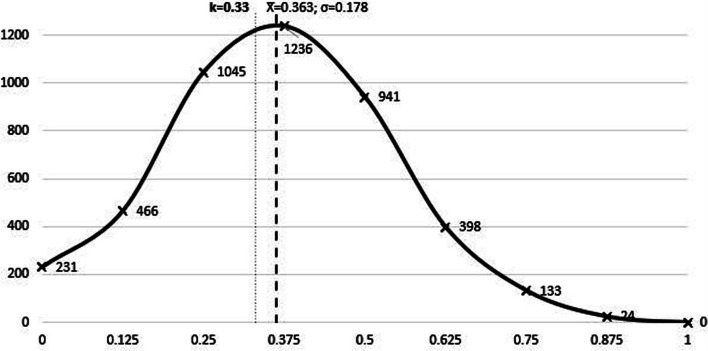
The poverty headcount was 61.06%, the average poverty gap 47.71%, the adjusted poverty headcount 29.13% and the average multidimensional poverty index was 0.363. Further, antenatal care utilization was regressive with respect to poverty. The regression analyses indicated that older women; being a widow (small number of widows (n = 3) asserts interpreting result with caution); or formally employed increase the likelihood of accessing antenatal care more often in pregnancy. Travelling for over an hour to receive care was negatively associated with utilization.
This study indicated high levels of multidimensional poverty in PNG and that ANC utilization was regressive; highlighting the need to encourage pregnant women, especially those who are economically more vulnerable to visit clinics regularly throughout pregnancy.
尽管过去十年全球贫困率有所下降,但亚太地区的贫困率下降速度相对较慢。贫困仍然是造成产妇和新生儿健康状况不佳的主要原因,也是及时获得产前护理的障碍。巴布亚新几内亚是亚太地区贫困率最高和产妇及新生儿结局最差的国家之一。在这种情况下,很少有研究调查产前护理利用方面的公平性。我们探讨了产前护理利用的公平性以及服务利用的决定因素,其中包括巴布亚新几内亚多维贫困的衡量标准。
为了探讨贫困与产前护理利用之间的关联,本研究使用了来自十组集群随机对照试验的数据。使用 Alkire-Foster 方法得出产前诊所就诊者的贫困人数、平均贫困差距、调整后的贫困人数和多维贫困指数。使用多维贫困指数探索服务利用的分布情况,然后进行多元回归分析,评估服务利用的决定因素。
贫困人数为 61.06%,平均贫困差距为 47.71%,调整后的贫困人数为 29.13%,平均多维贫困指数为 0.363。此外,产前护理利用与贫困呈负相关。回归分析表明,年龄较大的妇女;丧偶(寡妇人数较少(n=3),谨慎解释结果);或正式就业增加了怀孕期间更频繁接受产前护理的可能性。前往诊所接受护理需要一个多小时的时间与利用情况呈负相关。
本研究表明巴布亚新几内亚多维贫困水平较高,而 ANC 利用率呈倒退趋势;这突显了鼓励孕妇,特别是那些经济上较为脆弱的孕妇,在整个怀孕期间定期到诊所就诊的必要性。