Tuxen Anna, Malmborg Morten, Nouravesh Nina, Videbaek Lars, Malik Mariam, Zahir Deewa, Koeber Lars, Andersen Camilla F, Butt Jawad H, Jensen Jesper, Foesbol Emil, Andersson Charlotte, Gustafsson Finn, Schou Morten
Department of Cardiology, Herlev and Gentofte University Hospital, Denmark.
Department of Cardiology, Odense University Hospital, Odense, Denmark.
Int J Cardiol Heart Vasc. 2024 Jun 8;53:101441. doi: 10.1016/j.ijcha.2024.101441. eCollection 2024 Aug.
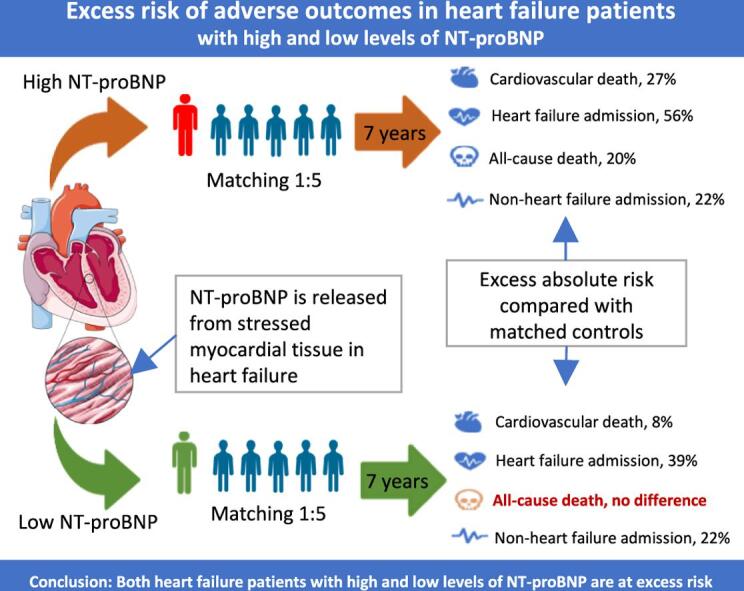
This study investigated excess risk in patients with heart failure with reduced left ventricular ejection fraction (HFrEF) with or without elevated levels of NT-proBNP (N-terminal pro-brain natriuretic peptide).
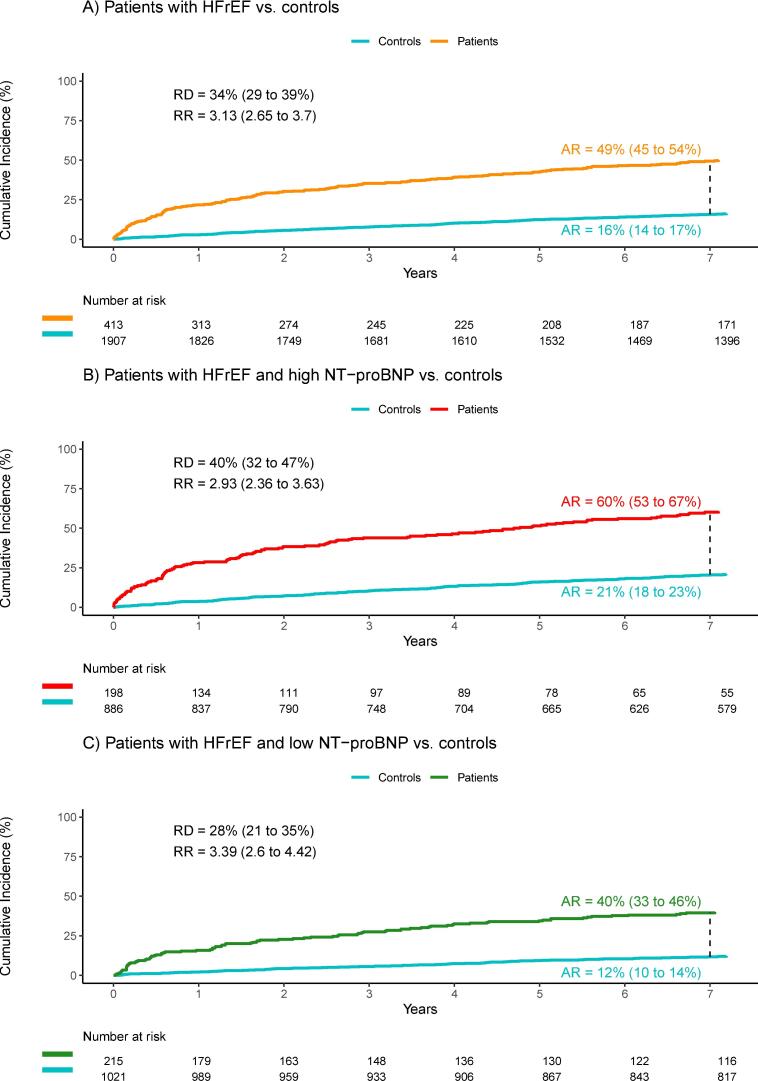
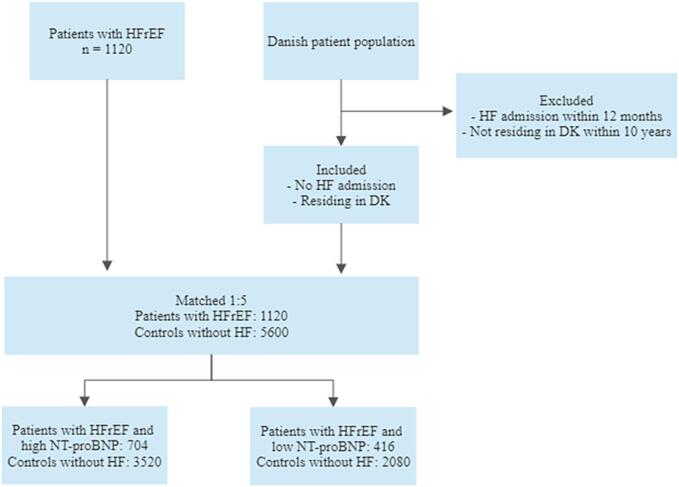
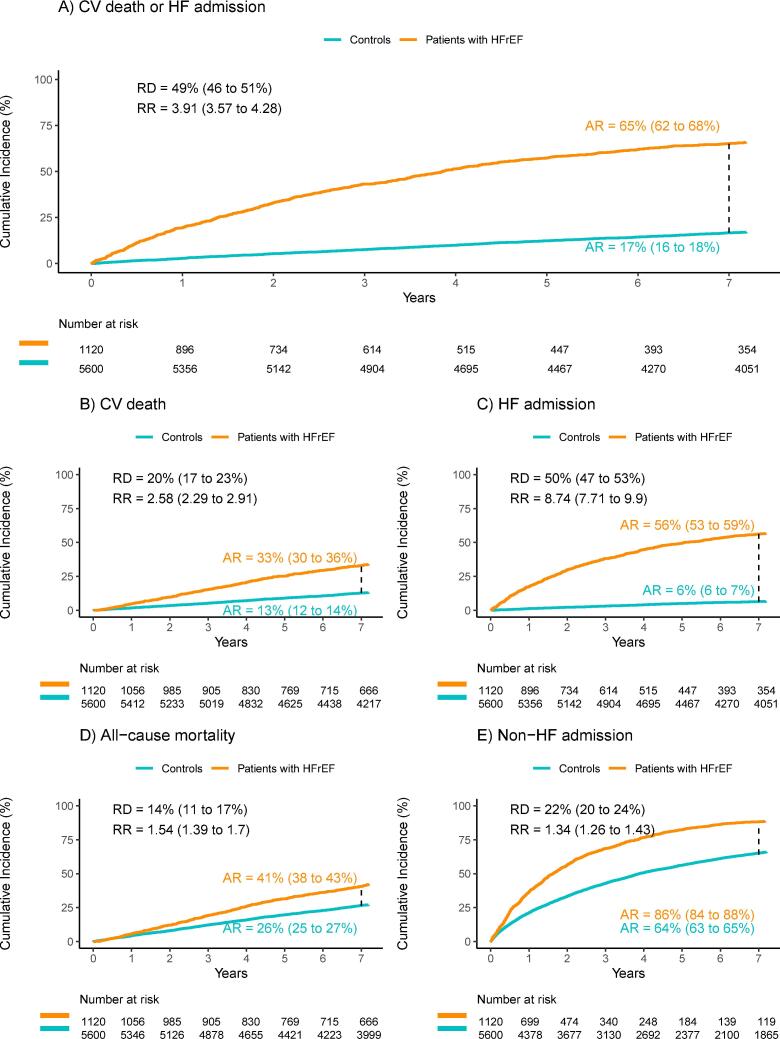
Patients with HFrEF from the NorthStar cohort (n = 1120) were matched on age, sex, and presence of AF (atrial fibrillation/flutter) to five controls without HFrEF from The Danish National Patient Registries. Patients were compared with controls before and after stratification according to baseline NT-proBNP levels, with cutoffs defined as </≥ 600 pg/ml in patients with sinus rhythm and </≥ 900 pg/ml in patients with AF. The primary composite endpoint was a 7-year risk of cardiovascular death or HF admission.
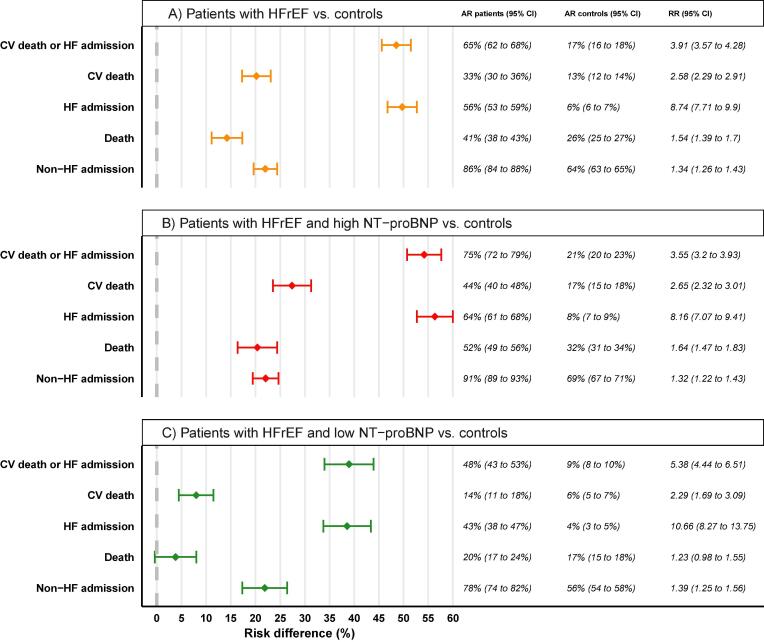
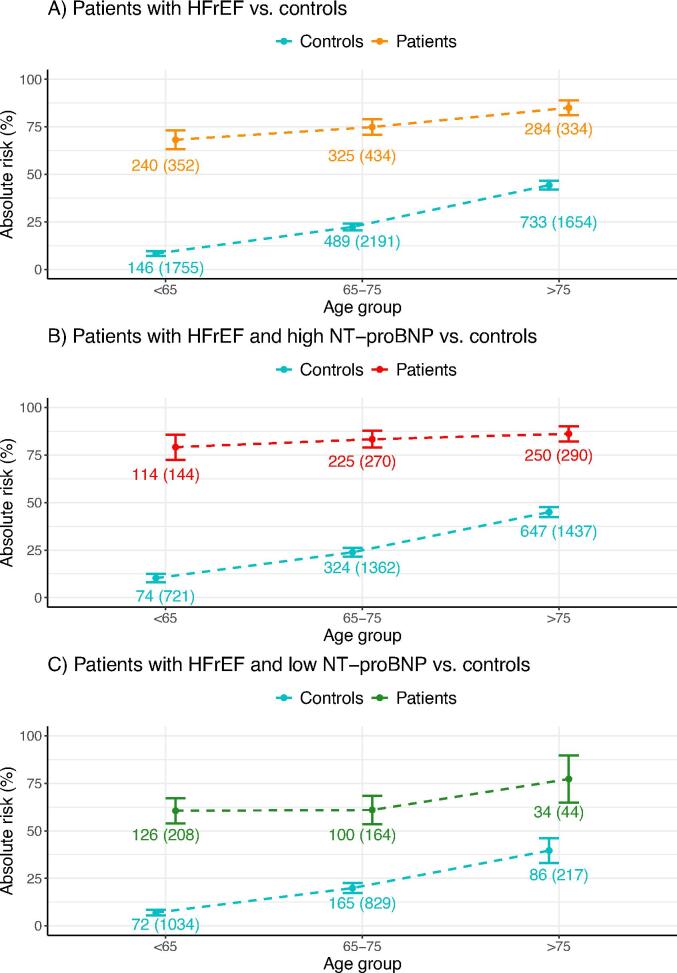
In the HFrEF cohort, 704 patients had high NT-proBNP (median age, 73; mean left ventricular ejection fraction (LVEF), 33%). 416 patients had low NT-proBNP (median age, 65; LVEF, 30%). Patients from both groups were in NYHA class I-III. The primary endpoint occurred in 531 patients (75.4%) with HFrEF and elevated NT-proBNP, and 748 controls (21.3%) (risk difference, 54.2%; 95% confidence interval (CI) 50.7-57.6%). In comparison, it occurred in 199 patients (47.9%) with HFrEF and without elevated NT-proBNP, and 185 controls (8,9%) (risk difference, 38.9%; 95% CI 34.0-43.9%). Risk differences for all secondary endpoints were significant, except for overall mortality in the low NT-proBNP group (risk difference, 3.8%; 95% CI, -0.4-8.0%).
This study identified a significant excess risk in patients with HFrEF across various endpoints, which persisted after stratification into high and low levels of NT-proBNP.
本研究调查了左心室射血分数降低的心力衰竭(HFrEF)患者中,无论NT-proBNP(N端脑钠肽前体)水平是否升高的额外风险。
来自北极星队列的1120例HFrEF患者,在年龄、性别和房颤(心房颤动/扑动)存在情况方面与丹麦国家患者登记处的5例无HFrEF的对照进行匹配。根据基线NT-proBNP水平进行分层前后,将患者与对照进行比较,窦性心律患者的临界值定义为</≥600 pg/ml,房颤患者的临界值定义为</≥900 pg/ml。主要复合终点是心血管死亡或心力衰竭住院的7年风险。
在HFrEF队列中,704例患者NT-proBNP水平较高(中位年龄73岁;平均左心室射血分数(LVEF)33%)。416例患者NT-proBNP水平较低(中位年龄65岁;LVEF 30%)。两组患者均处于纽约心脏协会I-III级。主要终点发生在531例(75.4%)HFrEF且NT-proBNP升高的患者和748例对照(21.3%)中(风险差异54.2%;95%置信区间(CI)50.7-57.6%)。相比之下,主要终点发生在199例(47.9%)HFrEF且NT-proBNP未升高的患者和185例对照(8.9%)中(风险差异38.9%;95%CI 34.0-43.9%)。除NT-proBNP水平较低组的全因死亡率外(风险差异3.8%;95%CI,-0.4-8.0%),所有次要终点的风险差异均具有统计学意义。
本研究发现HFrEF患者在各个终点均存在显著的额外风险,在分层为NT-proBNP高水平和低水平后该风险仍然存在。