School of Population Health, University of New South Wales, Sydney, Australia.
Department of Family and Community Health, Fred N. Binka School of Public Health, University of Health and Allied Sciences, Hohoe, Ghana.
BMC Health Serv Res. 2024 Sep 4;24(1):1026. doi: 10.1186/s12913-024-11261-z.
Between 2006 and 2017, antenatal care (ANC) coverage in Benin declined, potentially exacerbating inequalities and substantiating the need for health inequality monitoring. This study examines inequalities in ANC attendance in Benin, disaggregated by women's age, educational level, economic status, place of residence, region of residence, and the extent to which they have changed over time.
Three rounds of the Benin Demographic and Health Surveys (2006, 2011-12, and 2017-18) were analyzed to examine inequalities in ANC coverage. An exploratory descriptive approach was adopted for the analysis. Simple [difference (D) and ratio (R)] and complex [population attributable risk (PAR) and population attributable fraction (PAF)] measures of inequalities were computed using the World Health Organization's Health Equity Assessment Toolkit (WHO's HEAT) online platform. The measures were computed separately for each of the three surveys, and their estimates were compared.
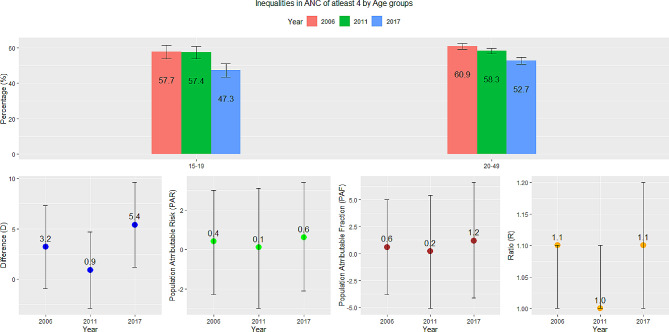
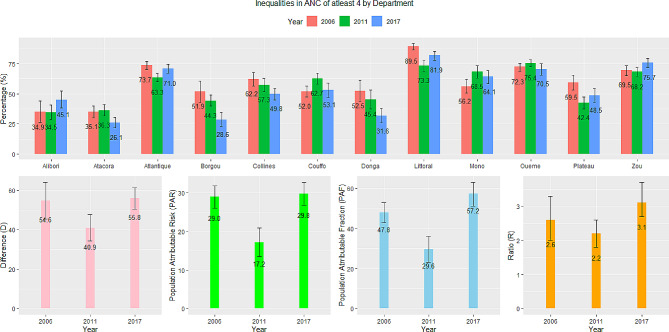
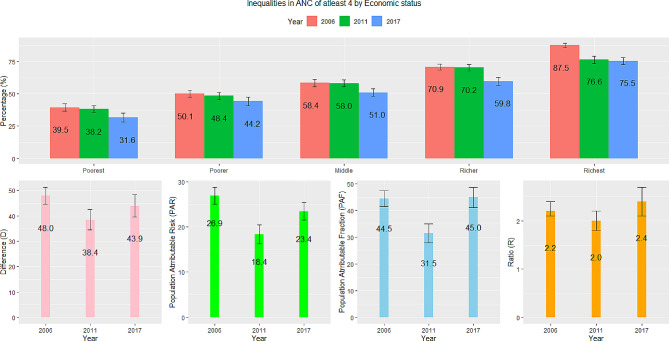
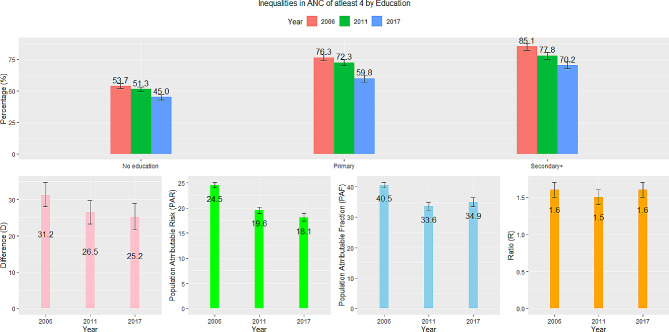
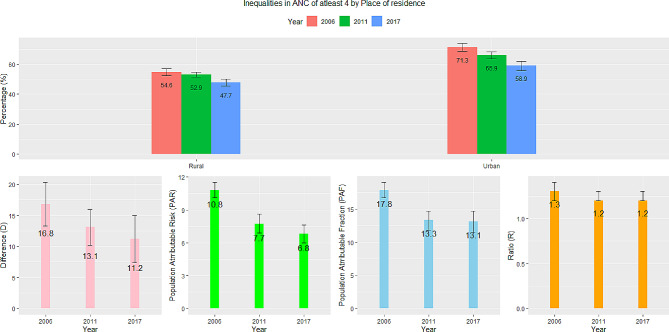
The findings revealed an 8.4% decline in at least four ANC visits between 2006 and 2017-18. The decline occurred irrespective of age, educational status, economic status, place of residence, and region. Region-related inequalities were the largest and increased slightly between 2006 (D = 54.6; R = 2.6; PAF = 47.8, PAR = 29.0) and 2017-18 (D = 55.8; R = 3.1; PAF = 57.2, PAR = 29.8). Education (2006: D = 31.3, R = 1.6, PAF = 40.5, PAR = 24.5; 2017-18: D = 25.2, R = 1.6, PAF = 34.9, PAR = 18.1) and rural-urban (2006: D = 16.8, R = 1.3, PAF = 17.8, PAR = 10.8; 2017-18: D = 11.2, R = 1.2, PAF = 13.1, PAR = 6.8) inequalities reduced while economic status inequalities did not improve (2006: D = 48, R = 2.2, PAF = 44.5, PAR = 26.9; 2017-18: D = 43.9, R = 2.4, PAF = 45.0, PAR = 23.4). Age inequalities were very minimal.
ANC inequalities remain deeply ingrained in Benin. Addressing their varying levels requires comprehensive strategies that encompass both supply-and demand-side interventions, focusing on reaching uneducated women in the poorest households and those residing in rural areas and Atacora.
2006 年至 2017 年间,贝宁的产前保健(ANC)覆盖率下降,这可能加剧了不平等现象,并证明需要对卫生不平等情况进行监测。本研究分析了贝宁 ANC 就诊的不平等现象,按妇女的年龄、教育水平、经济状况、居住地点、居住地区以及随时间变化的程度进行了分类。
对三轮贝宁人口与健康调查(2006 年、2011-12 年和 2017-18 年)进行分析,以研究 ANC 覆盖率的不平等情况。采用探索性描述性方法进行分析。使用世界卫生组织(WHO)的卫生公平评估工具包(WHO 的 HEAT)在线平台计算了简单(差异(D)和比值(R))和复杂(人群归因风险(PAR)和人群归因分数(PAF))不平等措施。分别为每一次调查计算了这些措施,并对其进行了比较。
研究结果显示,2006 年至 2017-18 年期间,至少接受四次 ANC 检查的比例下降了 8.4%。这一下降与年龄、教育状况、经济状况、居住地点和地区无关。与地区相关的不平等现象最大,并在 2006 年(D=54.6;R=2.6;PAF=47.8,PAR=29.0)和 2017-18 年(D=55.8;R=3.1;PAF=57.2,PAR=29.8)略有增加。教育(2006 年:D=31.3,R=1.6,PAF=40.5,PAR=24.5;2017-18 年:D=25.2,R=1.6,PAF=34.9,PAR=18.1)和城乡(2006 年:D=16.8,R=1.3,PAF=17.8,PAR=10.8;2017-18 年:D=11.2,R=1.2,PAF=13.1,PAR=6.8)不平等现象减少,而经济地位不平等现象并未改善(2006 年:D=48,R=2.2,PAF=44.5,PAR=26.9;2017-18 年:D=43.9,R=2.4,PAF=45.0,PAR=23.4)。年龄不平等现象非常微小。
ANC 不平等现象在贝宁仍然根深蒂固。解决这些不平等现象的不同程度需要综合的策略,包括供需两方面的干预措施,重点是覆盖未受教育的贫困家庭妇女以及居住在农村地区和阿塔科拉的妇女。