Wang Qin, Zeng Yaqing, Jiao Linna, He Jianli, Li Baoyi, Guo Yihua, Song Zhibin
Department of Neurology, Xiaolan People's Hospital of Zhongshan, Zhongshan, China.
Front Neurol. 2024 Aug 21;15:1456559. doi: 10.3389/fneur.2024.1456559. eCollection 2024.
Several recent clinical studies have indicated that vamorolone is comparable in effectiveness to glucocorticosteroids for treating Duchenne muscular dystrophy (DMD). However, there is a lack of extensive data regarding the efficacy and safety of various doses of vamorolone. We conducted a study to evaluate the efficacy of different doses of vamorolone in boys with DMD, and compare the safety of vamorolone vs. glucocorticosteroids, prednisone or deflazacort in boys with DMD.
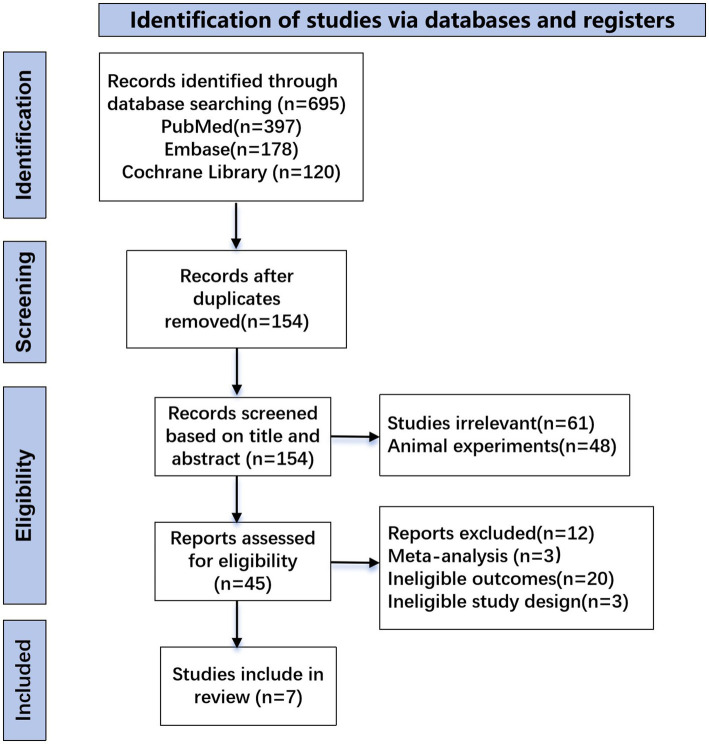
We performed systematic searches of the PubMed, Embase, and Cochrane Library databases for vamorolone, glucocorticosteroids, prednisone or deflazacort in boys with DMD. We assessed statistical heterogeneity across trials based on the Newcastle Ottawa scale (NOS) tool test and I values, and mean differences were pooled using the random-effects model. We used traditional meta-analysis to evaluate efficacy and safety of vamorolone 6.0 mg/kg/d vs. vamorolone 2.0 mg/kg/d and vamorolone vs. prednisone. A network meta-analysis was applied to estimated the safety of vamorolone in comparison to glucocorticosteroids, prednisone and deflazacort. Our meta-analysis were performed using Revman 5.4 software, and our network meta-analysis were performed using Stata/MP 18.0.
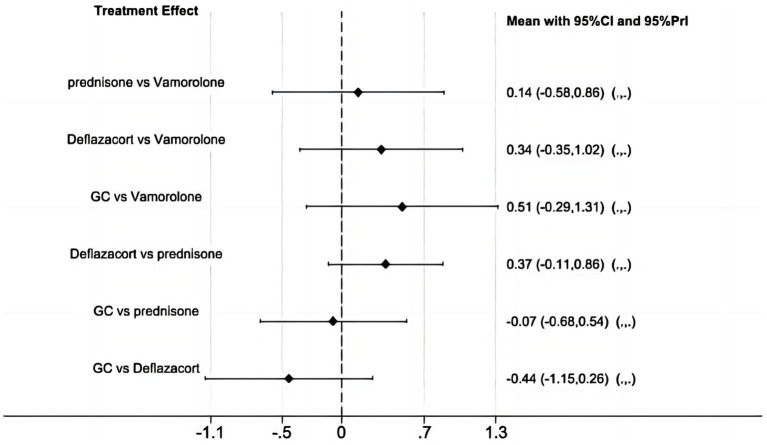
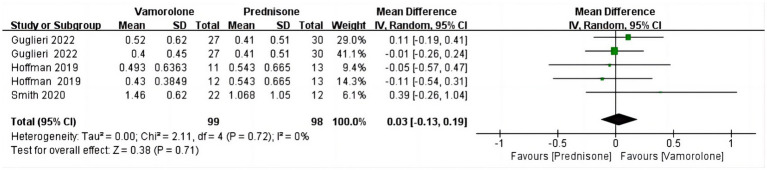
In the meta-analysis, a total of 193 patients were analyzed across four clinical trials (97 patients receiving vamorolone 2 mg/kg per day; 96 patients receiving vamorolone 2 mg/kg per day). We observed that there were statistically significant differences in boys with DMD between vamorolone 6.0 mg/kg/d and vamorolone 2.0 mg/kg/d in TTSTANDV (MD = 0.03, 95%CI = 0.00-0.06, = 0.04), TTRWV (MD = 0.13, 95%CI = 0.08-0.19, < 0.01), 6MWT (MD = 24.54, 95%CI = 4.46-44.82, = 0.02), TTCLIMBV (MD = 0.04, 95%CI = 0.01-0.06, = 0.009), no significant difference in BMI z score (MD = 0.09, 95%CI = -0.03-0.20, = 0.13). Indirect comparisons derived from network meta-analysis did not show significant differences among vamorolone, glucocorticosteroids, prednisone and deflazacort in BMI z score.
Our findings implied that boys with DMD who took vamorolone 6 mg/kg daily instead of 2 mg/kg daily may be safer and have superior motor function. However, more large sample randomized controlled trials are needed to confirm our results.
This systematic review and meta-analysis has been registered in the International Prospective Register of Ongoing Systematic Reviews PROSPERO (registration number: CRD42024562916).
近期多项临床研究表明,在治疗杜氏肌营养不良症(DMD)方面,万莫洛龙的疗效与糖皮质激素相当。然而,关于不同剂量万莫洛龙的疗效和安全性,目前缺乏广泛的数据。我们开展了一项研究,以评估不同剂量万莫洛龙对DMD男孩的疗效,并比较万莫洛龙与糖皮质激素、泼尼松或地夫可特在DMD男孩中的安全性。
我们对PubMed、Embase和Cochrane图书馆数据库进行了系统检索,查找有关DMD男孩使用万莫洛龙、糖皮质激素、泼尼松或地夫可特的研究。我们基于纽卡斯尔渥太华量表(NOS)工具测试和I值评估各试验间的统计异质性,并使用随机效应模型汇总平均差异。我们采用传统荟萃分析来评估6.0mg/kg/d万莫洛龙与2.0mg/kg/d万莫洛龙以及万莫洛龙与泼尼松的疗效和安全性。应用网络荟萃分析来估计万莫洛龙与糖皮质激素、泼尼松和地夫可特相比的安全性。我们使用Revman 5.4软件进行荟萃分析,使用Stata/MP 18.0进行网络荟萃分析。
在荟萃分析中,四项临床试验共分析了193例患者(97例患者每天接受2mg/kg万莫洛龙治疗;96例患者每天接受2mg/kg万莫洛龙治疗)。我们观察到,在DMD男孩中,6.0mg/kg/d万莫洛龙与2.0mg/kg/d万莫洛龙在TTSTANDV(MD = 0.03,95%CI = 0.00 - 0.06,P = 0.04)、TTRWV(MD = 0.13,95%CI = 0.08 - 0.19,P < 0.01)、6MWT(MD = 24.54,95%CI = 4.46 - 44.82,P = 0.02)、TTCLIMBV(MD = 0.04,95%CI = 0.01 - 0.06,P = 0.009)方面存在统计学显著差异,BMI z评分无显著差异(MD = 0.09,95%CI = -0.03 - 0.20,P = 0.13)。网络荟萃分析得出的数据间接比较结果显示,万莫洛龙、糖皮质激素、泼尼松和地夫可特在BMI z评分方面无显著差异。
我们的研究结果表明,每天服用6mg/kg万莫洛龙而非2mg/kg万莫洛龙的DMD男孩可能更安全且运动功能更优。然而,需要更多大样本随机对照试验来证实我们的结果。
本系统评价和荟萃分析已在国际前瞻性系统评价注册库PROSPERO中注册(注册号:CRD42024562916)。