Clark Andrew, Prakash Manyu, Chabria Shiven, Pierce Amy, Castillo-Mancilla Jose R, Wang Marcia, Du Fangfang, Tenorio Allan R
ViiV Healthcare, Brentford, UK.
ViiV Healthcare, Branford, Connecticut, USA.
Open Forum Infect Dis. 2024 Aug 26;11(9):ofae469. doi: 10.1093/ofid/ofae469. eCollection 2024 Sep.
Fostemsavir, a first-in-class attachment inhibitor that binds to the viral envelope protein gp120, is approved for heavily treatment-experienced persons with HIV-1 with limited treatment options. We explored changes in immunologic and coagulopathy parameters in the BRIGHTE study: a phase 3 trial that evaluated fostemsavir plus optimized background therapy in heavily treatment-experienced adults with multidrug-resistant HIV-1.
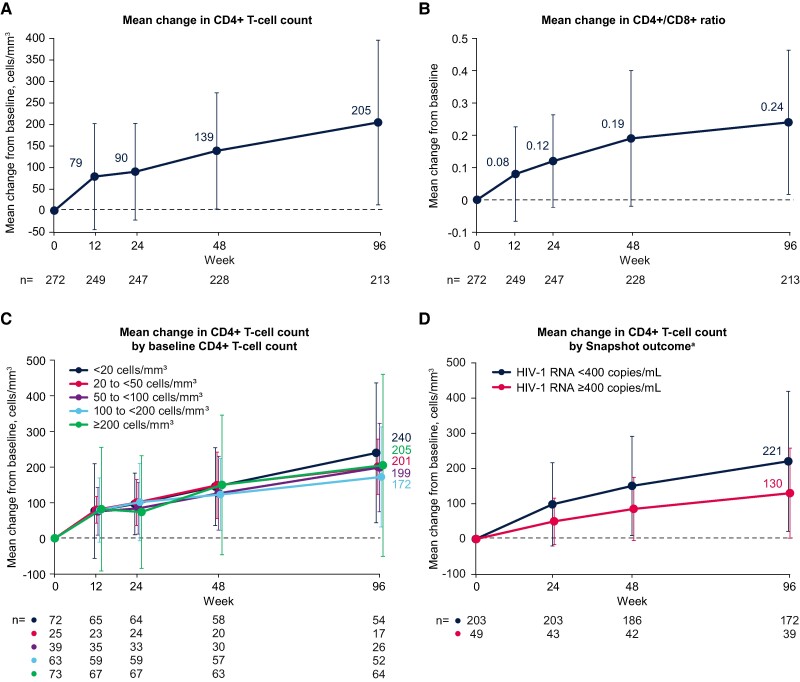
CD4+ T-cell count, CD4+/CD8+ ratio, soluble CD14, soluble CD163, and D-dimer levels were measured through 96 weeks in participants with 1 or 2 fully active antiretroviral agents available at screening. No formal statistical analyses were performed.
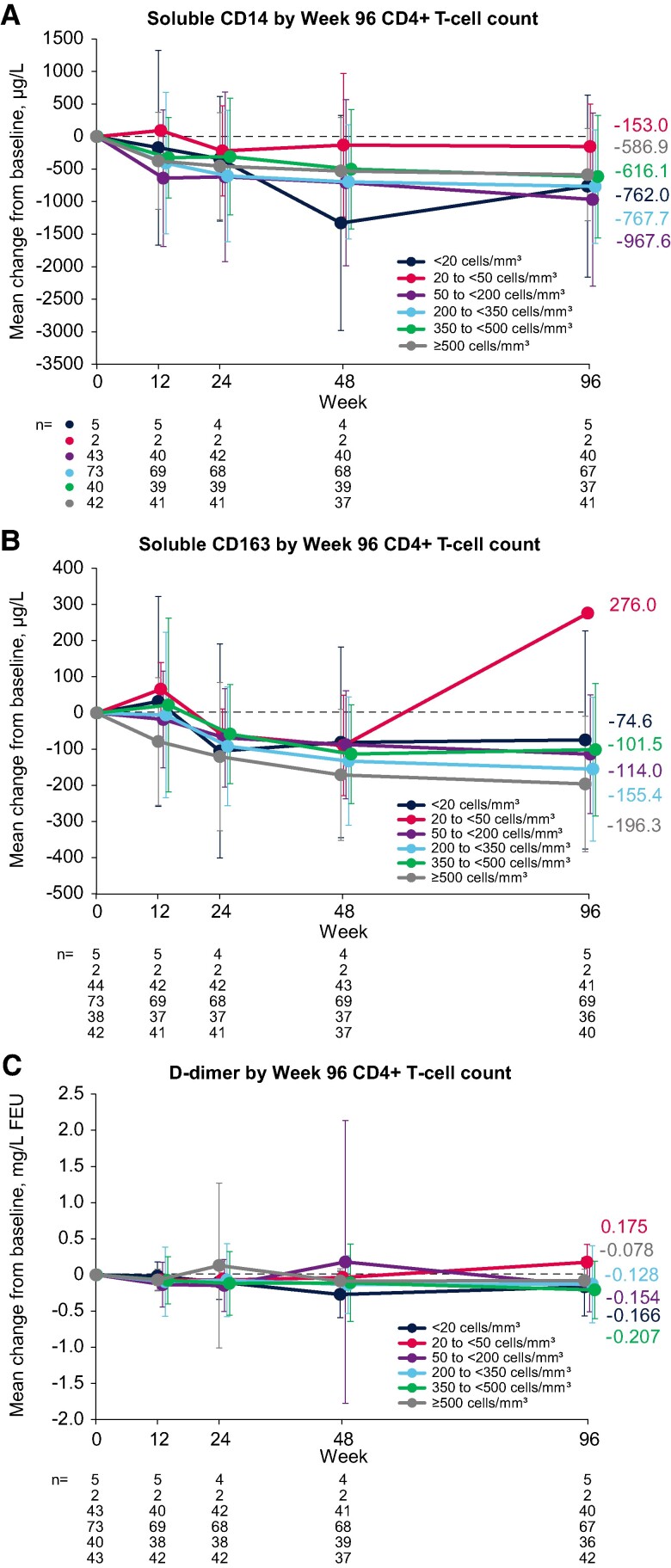
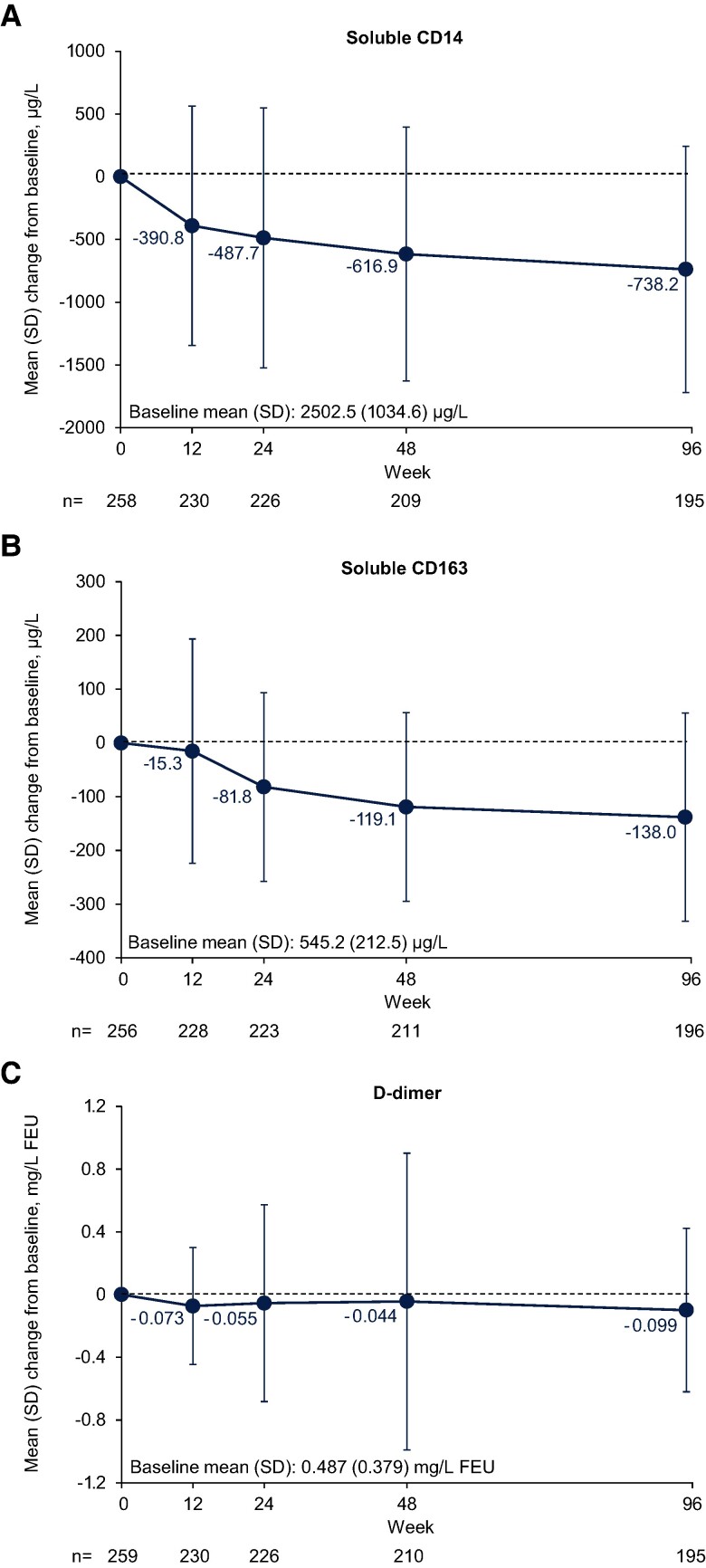
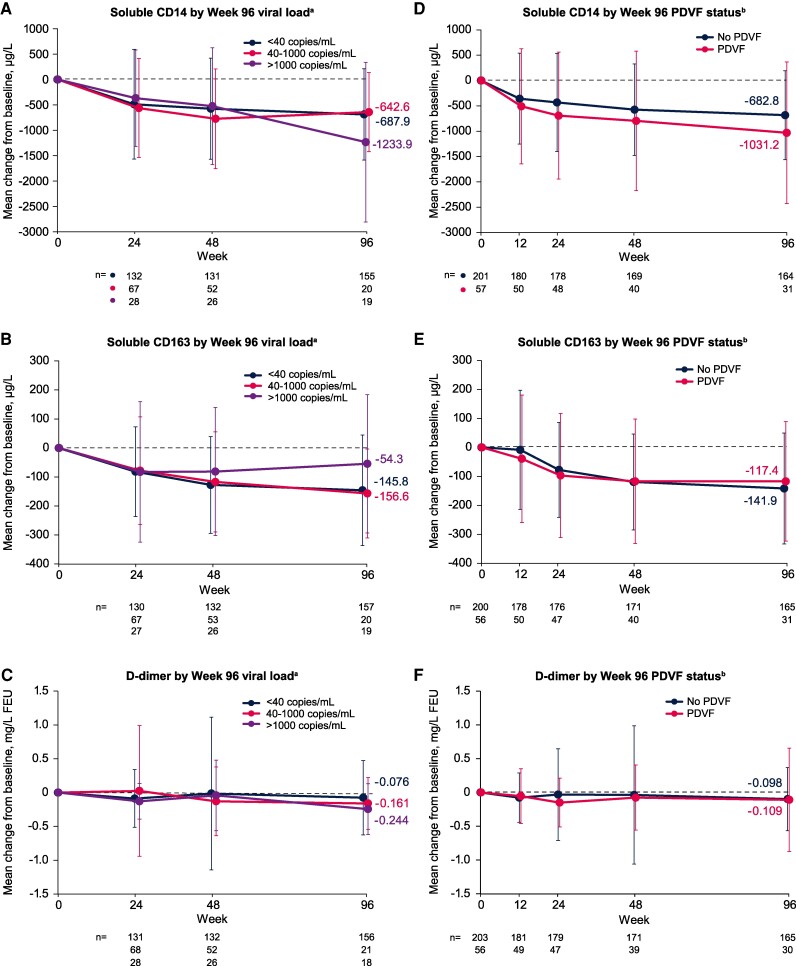
Among 272 participants, increases were observed from baseline to week 96 in CD4+ T-cell count (mean increase, +205 cells/mm) and CD4+/CD8+ ratio (mean increase, +0.24). The proportion of observed participants with a CD4+/CD8+ ratio ≥0.45 increased from 9% (25/272) at baseline to 40% (85/213) at week 96. From baseline to week 96, we also observed trends toward decreases in the following (mean [SD] change): soluble CD14, -738.2 (981.8) µg/L; soluble CD163, -138.0 (193.4) µg/L; and D-dimer, -0.099 (0.521) mg/L fibrinogen-equivalent units. Decreases in biomarkers were generally observed among subgroups by baseline disease characteristics, virologic response, and CD4+ T-cell count.
These data suggest that heavily treatment-experienced persons with multidrug-resistant HIV-1 treated with fostemsavir + optimized background therapy may have improvements in immune parameters, including markers of monocyte activation and coagulopathy.
NCT02362503 (ClinicalTrials.gov; https://clinicaltrials.gov/study/NCT02362503).
福斯特韦尔是一种一流的附着抑制剂,可与病毒包膜蛋白gp120结合,已被批准用于治疗经历丰富但治疗选择有限的HIV-1感染者。我们在BRIGHTE研究中探索了免疫和凝血病参数的变化:这是一项3期试验,评估了福斯特韦尔联合优化背景疗法用于治疗经历丰富的多药耐药HIV-1成年患者。
在筛查时可获得1种或2种完全有效的抗逆转录病毒药物的参与者中,测量其96周内的CD4+ T细胞计数、CD4+/CD8+比值、可溶性CD14、可溶性CD163和D-二聚体水平。未进行正式的统计分析。
在272名参与者中,观察到从基线到第96周CD4+ T细胞计数(平均增加+205个细胞/mm³)和CD4+/CD8+比值(平均增加+0.24)有所增加。CD CD4+/CD8+比值≥0.45的参与者比例从基线时的9%(25/272)增加到第96周时的40%(85/213)。从基线到第96周,我们还观察到以下指标有下降趋势(平均[标准差]变化):可溶性CD14,-738.2(981.8)μg/L;可溶性CD163,-138.0(193.4)μg/L;以及D-二聚体,-0.099(0.521)mg/L纤维蛋白原当量单位。根据基线疾病特征、病毒学反应和CD4+ T细胞计数,在各亚组中普遍观察到生物标志物下降。
这些数据表明,接受福斯特韦尔+优化背景疗法治疗的多药耐药HIV-1治疗经历丰富的患者,其免疫参数可能会得到改善,包括单核细胞激活和凝血病标志物。
NCT02362503(ClinicalTrials.gov;https://clinicaltrials.gov/study/NCT02362503)。