Crescioli Elena, Nielsen Frederik Mølgaard, Bunzel Anne-Marie, Eriksen Anne Sofie Broberg, Siegemund Martin, Poulsen Lone Musaeus, Andreasen Anne Sofie, Bestle Morten Heiberg, Iversen Susanne Andi, Brøchner Anne Craveiro, Grøfte Thorbjørn, Hildebrandt Thomas, Laake Jon Henrik, Kjær Maj-Brit Nørregaard, Lange Theis, Perner Anders, Klitgaard Thomas Lass, Schjørring Olav Lilleholt, Rasmussen Bodil Steen
Department of Anaesthesia and Intensive Care, Aalborg University Hospital, Hobrovej 18-22, 9100, Aalborg, Denmark.
Department of Clinical Medicine, Aalborg University, Aalborg, Denmark.
Intensive Care Med. 2024 Oct;50(10):1603-1613. doi: 10.1007/s00134-024-07613-2. Epub 2024 Sep 5.
The aim of this study was to evaluate one-year outcomes of lower versus higher oxygenation targets in intensive care unit (ICU) patients with coronavirus disease 2019 (COVID-19) and severe hypoxaemia.
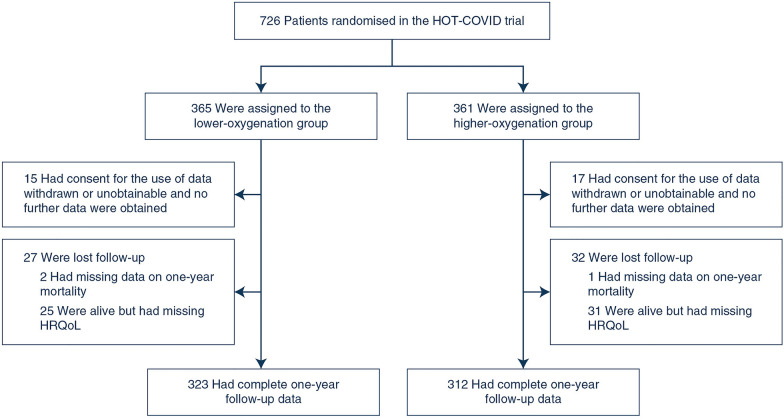
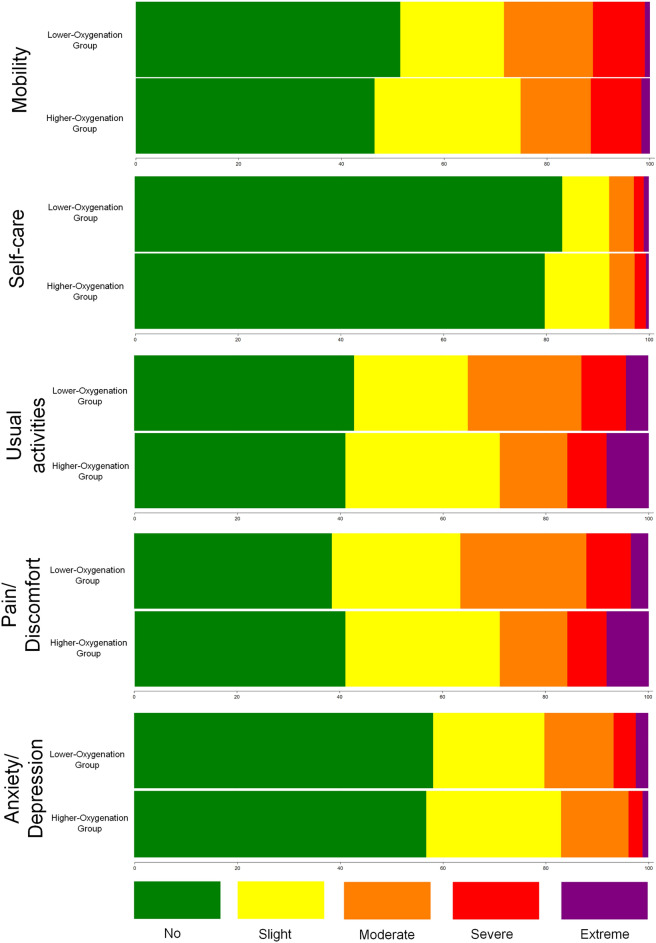
We conducted pre-planned analyses of one-year mortality and health-related quality of life (HRQoL) in the Handling Oxygenation Targets in COVID-19 trial. The trial randomised 726 ICU patients with COVID-19 and hypoxaemia to partial pressure of arterial oxygen targets of 8 kPa (60 mmHg) versus 12 kPa (90 mmHg) during ICU stay up to 90 days, including readmissions. HRQoL was assessed using EuroQol visual analogue scale (EQ-VAS) and 5-level 5-dimension questionnaire (EQ-5D-5L). Outcomes were analysed in the intention-to-treat population. Non-survivors were assigned the worst possible score (zero), and multiple imputation was applied for missing EQ-VAS values.
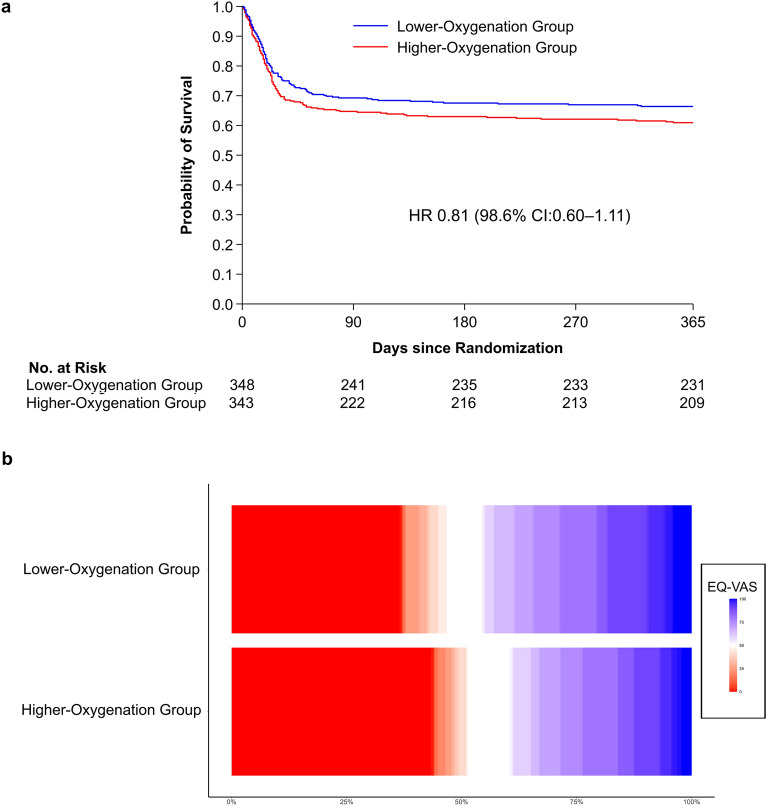
We obtained one-year vital status for 691/726 (95.2%) of patients and HRQoL data for 642/726 (88.4%). At one year, 117/348 (33.6%) of patients in the lower-oxygenation group had died compared to 134/343 (39.1%) in the higher-oxygenation group (adjusted risk ratio: 0.85; 98.6% confidence interval (CI) 0.66-1.09; p = 0.11). Median EQ-VAS was 50 (interquartile range, 0-80) versus 40 (0-75) (adjusted mean difference: 4.8; 98.6% CI - 2.2 to 11.9; p = 0.09) and EQ-5D-5L index values were 0.61 (0-0.81) in the lower-oxygenation group versus 0.43 (0-0.79) (p = 0.20) in the higher-oxygenation group, respectively.
Among adult ICU patients with COVID-19 and severe hypoxaemia, one-year mortality results were most compatible with benefit of the lower oxygenation target, which did not appear to result in more survivors with poor quality of life.
本研究旨在评估2019冠状病毒病(COVID-19)合并严重低氧血症的重症监护病房(ICU)患者,较低与较高氧合目标的一年期预后。
我们对COVID-19试验中处理氧合目标的一年期死亡率和健康相关生活质量(HRQoL)进行了预先计划的分析。该试验将726例患有COVID-19和低氧血症的ICU患者随机分为两组,在长达90天的ICU住院期间(包括再次入院),动脉血氧分压目标分别为8 kPa(60 mmHg)和12 kPa(90 mmHg)。使用欧洲五维度健康量表视觉模拟量表(EQ-VAS)和5级5维度问卷(EQ-5D-5L)评估HRQoL。在意向性治疗人群中分析结果。非幸存者被赋予最差可能分数(零),并对缺失的EQ-VAS值应用多重填补法。
我们获得了691/726(95.2%)患者的一年期生命状态数据和642/726(88.4%)患者的HRQoL数据。一年时,低氧合组117/348(33.6%)的患者死亡,而高氧合组为134/343(39.1%)(调整风险比:0.85;98.6%置信区间(CI)0.66 - 1.09;p = 0.11)。EQ-VAS中位数分别为50(四分位间距,0 - 80)和40(0 - 75)(调整平均差:4.8;98.6% CI - 2.2至11.9;p = 0.09),低氧合组和高氧合组的EQ-5D-5L指数值分别为0.61(0 - 0.81)和0.43(0 - 0.79)(p = 0.20)。
在患有COVID-19和严重低氧血症的成年ICU患者中,一年期死亡率结果最符合较低氧合目标的益处,且较低氧合目标似乎不会导致更多生活质量差的幸存者。