Verstraeten Laure M G, Reijnierse Esmee M, Spoelstra Thom, Meskers Carel G M, Maier Andrea B
Department of Human Movement Sciences, @AgeAmsterdam, Faculty of Behavioural and Movement Sciences, Amsterdam Movement Sciences, Vrije Universiteit, Amsterdam, The Netherlands.
Department of Medicine and Aged Care, @AgeMelbourne, The Royal Melbourne Hospital, The University of Melbourne, Melbourne, Victoria, Australia.
J Cachexia Sarcopenia Muscle. 2024 Oct;15(5):2094-2103. doi: 10.1002/jcsm.13557. Epub 2024 Sep 5.
Regaining walking ability is a key target in geriatric rehabilitation. This study evaluated the prevalence of walking ability at (pre-)admission and related clinical characteristics in a cohort of geriatric rehabilitation inpatients; in inpatients without walking ability, feasibility and effectiveness of progressive resistance exercise training (PRT) were assessed.
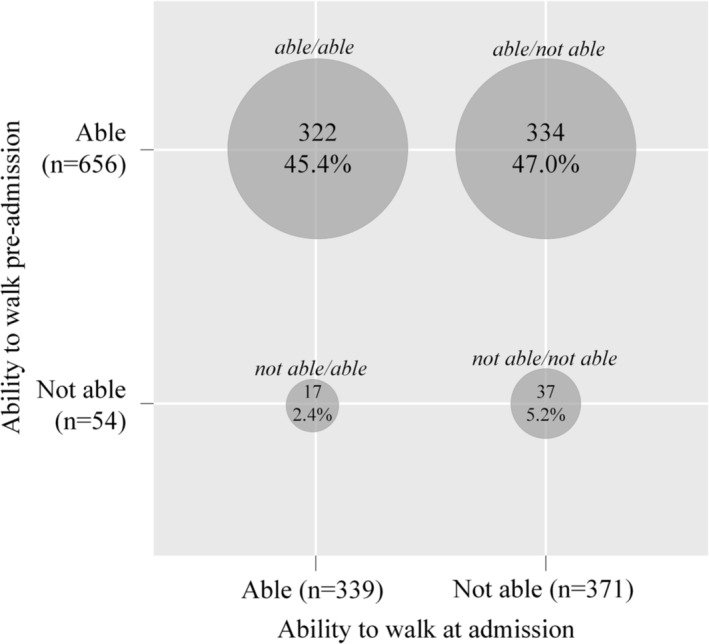
Inpatients within RESORT, an observational, longitudinal cohort of geriatric rehabilitation inpatients, were stratified in those with and without ability to walk independently (defined by Functional Ambulation Classification (FAC) score ≤ 2) at admission; further subdivision was performed by pre-admission walking ability. Clinical characteristics at admission, length of stay, and changes in physical and functional performance throughout admission were compared depending on (pre-)admission walking ability. Feasibility (relative number of PRT sessions given and dropout rate) and effectiveness [change in Short Physical Performance Battery, FAC, independence in (instrumental) activities of daily living (ADL/IADL)] of PRT (n = 11) in a subset of inpatients without ability to walk independently at admission (able to walk pre-admission) were investigated compared with usual care (n = 11) (LIFT-UP study).
Out of 710 inpatients (median age 83.5 years; 58.0% female), 52.2% were not able to walk independently at admission, and 7.6% were not able to walk pre-admission. Inpatients who were not able to walk independently at admission, had a longer length of stay, higher prevalence of cognitive impairment and frailty and malnutrition risk scores, and a lower improvement in independence in (I)ADL compared with inpatients who were able to walk at both admission and pre-admission. In LIFT-UP, the relative median number of PRT sessions given compared with the protocol (twice per weekday) was 11 out of 44. There were no dropouts. PRT improved FAC (P = 0.028) and ADL (P = 0.034) compared with usual care.
High prevalence of inpatients who are not able to walk independently and its negative impact on independence in (I)ADL during geriatric rehabilitation highlights the importance of tailored interventions such as PRT, which resulted in improvement in FAC and ADL.
恢复行走能力是老年康复的关键目标。本研究评估了老年康复住院患者入院时(入院前)行走能力的患病率及相关临床特征;对于无行走能力的住院患者,评估了渐进性抗阻运动训练(PRT)的可行性和有效性。
在RESORT研究中,将老年康复住院患者的观察性纵向队列中的患者,根据入院时能否独立行走(根据功能性步行分类(FAC)评分≤2定义)进行分层;再根据入院前行走能力进一步细分。根据入院时(入院前)行走能力,比较入院时的临床特征、住院时间以及整个住院期间身体和功能表现的变化。在入院时无独立行走能力(入院前能行走)的住院患者亚组中,研究了PRT(n = 11)与常规护理(n = 11)相比的可行性(给予的PRT疗程相对数量和退出率)和有效性[简短身体功能量表、FAC、(工具性)日常生活活动(ADL/IADL)独立性的变化](LIFT-UP研究)。
在710名住院患者中(中位年龄83.5岁;58.0%为女性),52.2%在入院时不能独立行走,7.6%在入院前不能行走。与入院时和入院前都能行走的住院患者相比,入院时不能独立行走的住院患者住院时间更长,认知障碍、衰弱和营养不良风险评分的患病率更高,(I)ADL独立性改善程度更低。在LIFT-UP研究中,与方案(每周工作日两次)相比,给予的PRT疗程相对中位数为44次中的11次。没有患者退出。与常规护理相比,PRT改善了FAC(P = 0.028)和ADL(P = 0.034)。
老年康复期间不能独立行走的住院患者患病率高,且对(I)ADL独立性有负面影响,这凸显了如PRT等针对性干预措施的重要性,PRT可改善FAC和ADL。