Department of Medical Sciences, Section of Neurosurgery, Uppsala University, Uppsala, Sweden.
Department of Surgical Sciences, Radiology, Uppsala University, Uppsala, Sweden.
Ups J Med Sci. 2024 Sep 3;129. doi: 10.48101/ujms.v129.10799. eCollection 2024.
Diffuse astrocytomas preferentially infiltrate eloquent areas affecting the outcome. A preoperative understanding of isocitrate dehydrogenase (IDH) status may offer opportunities for specific targeted therapies impacting treatment management. The aim of this study was to analyze clinical, topographical, radiological in WHO 2 astrocytomas with different IDH status and the long-term patient's outcome.
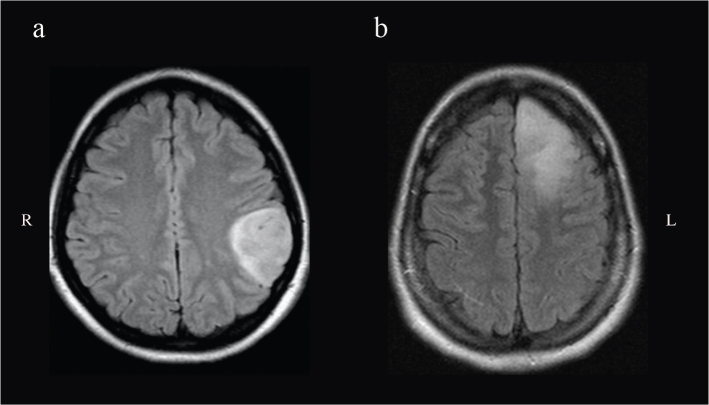
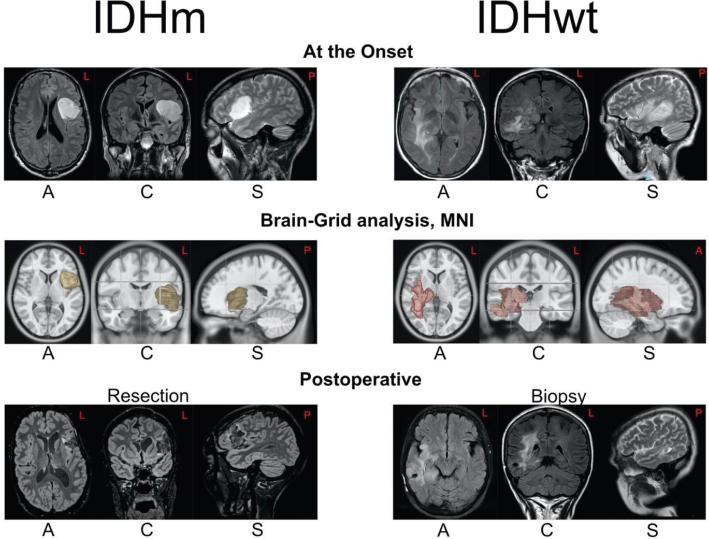
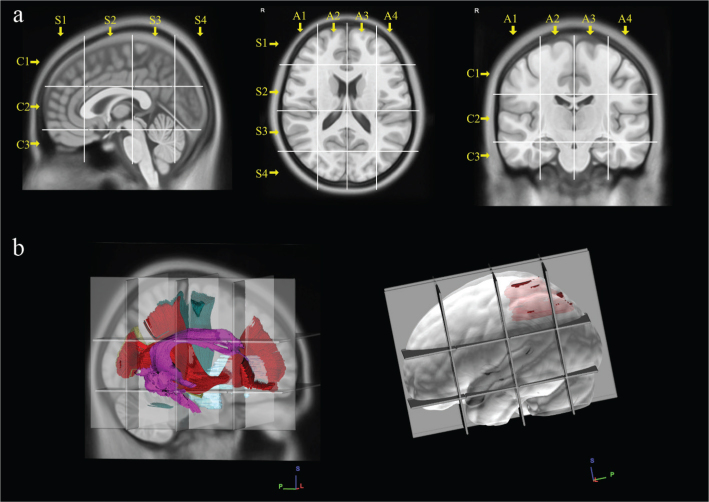
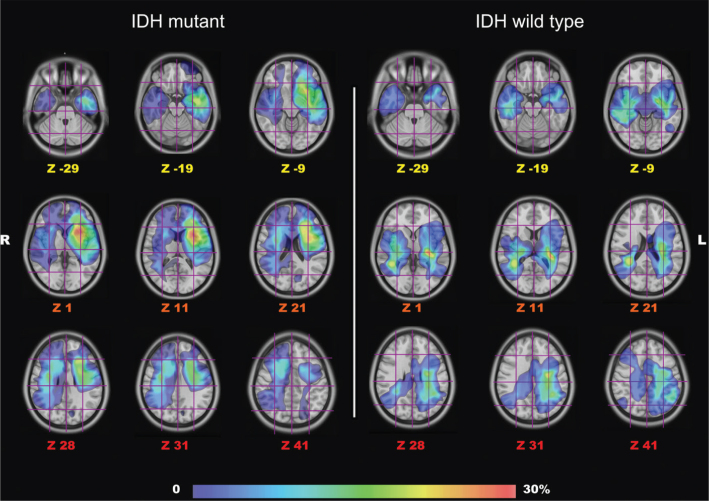
A series of confirmed WHO 2 astrocytoma patients (between 2005 and 2015) were retrospectively analyzed. MRI sequences (FLAIR) were used for tumor volume segmentation and to create a frequency map of their locations into the Montreal Neurological Institute (MNI) space. The Brain-Grid (BG) system (standardized radiological tool of intersected lines according to anatomical landmarks) was used as an overlay for infiltration analysis of each tumor. Long-term follow-up was used to perform a survival analysis.
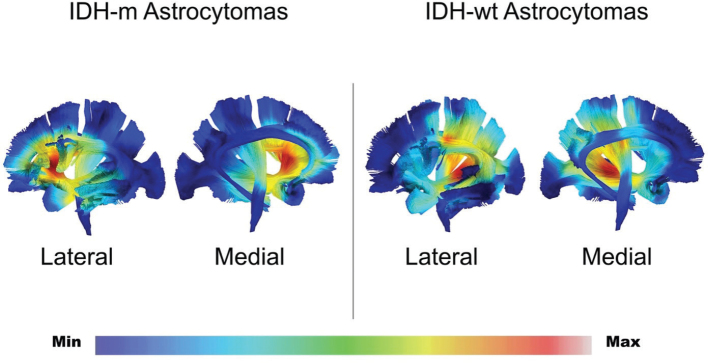
Forty patients with confirmed IDH status (26 IDH-mutant, IDHm/14 IDH-wild type, IDHwt) according to WHO 2021 classification were included with a mean follow-up of 7.8 years. IDHm astrocytomas displayed a lower number of BG-voxels ( < 0.05) and were preferentially located in the anterior insular region. IDHwt group displayed a posterior insular and peritrigonal location. IDHwt group displayed a shorter OS compared with IDHm ( < 0.05), with the infiltration of 7 or more BG-voxels as an independent factor predicting a shorter OS.
IDHm and IDHwt astrocytomas differed in preferential location, number of BG-voxels and OS at long follow-up time. The number of BG-voxels affected the OS in IDHwt was possibly reflecting higher tumor invasiveness. We encourage the systematic use of alternative observational tools, such as gradient maps and the Brain-Grid analysis, to better detect differences of tumor invasiveness in diffuse low-grade gliomas subtypes.
弥漫性星形细胞瘤优先浸润功能区,影响预后。术前了解异柠檬酸脱氢酶(IDH)状态可能为特定的靶向治疗提供机会,从而影响治疗管理。本研究旨在分析不同 IDH 状态的 WHO 2 级星形细胞瘤的临床、解剖和影像学特征,并对长期患者预后进行分析。
回顾性分析了一系列确诊的 WHO 2 级星形细胞瘤患者(2005 年至 2015 年期间)。采用 MRI 序列(FLAIR)对肿瘤体积进行分割,并在蒙特利尔神经学研究所(MNI)空间创建肿瘤位置的频率图。脑格(BG)系统(根据解剖学标志的交叉线的标准化放射学工具)用于对每个肿瘤的浸润进行分析。长期随访用于进行生存分析。
根据 2021 年 WHO 分类,共纳入 40 例 IDH 状态明确(26 例 IDH 突变型,IDHm/14 例 IDH 野生型,IDHwt)的患者,平均随访 7.8 年。IDHm 星形细胞瘤的 BG 体素数量较少(<0.05),并且优先位于前岛叶区。IDHwt 组显示后岛叶和旁角回区位置。与 IDHm 相比,IDHwt 组的 OS 较短(<0.05),7 个或更多 BG 体素的浸润是 OS 较短的独立预测因素。
在长期随访中,IDHm 和 IDHwt 星形细胞瘤在优先位置、BG 体素数量和 OS 方面存在差异。IDHwt 组的 BG 体素数量影响 OS,可能反映了肿瘤侵袭性较高。我们鼓励系统地使用替代观察工具,如梯度图和脑格分析,以更好地检测弥漫性低级别胶质瘤亚型的肿瘤侵袭性差异。