Hoang Marjorie T Q, Koh Ye Xin, Sultana Rehena, Allen John C, Moris Dimitrios, Cheow Peng Chung, Chung Alexander Y F, Jeyaraj Prema Raj, Mack Peter O P, Ooi London Lucien P J, Tan Ek Khoon, Teo Jin Yao, Kam Juinn Huar, Moe Fiona N N, Chua Jacelyn S S, Ng Ashley W Y, Goh Jade S Q, Goh Brian K P, Zani Sabino, Chow Pierce K H
Department of Hepatopancreatobiliary and Transplant Surgery, Division of Surgery and Surgical Oncology, Singapore General Hospital and National Cancer Centre Singapore.
Duke-NUS Medical School.
Int J Surg. 2024 Nov 1;110(11):7058-7066. doi: 10.1097/JS9.0000000000001868.
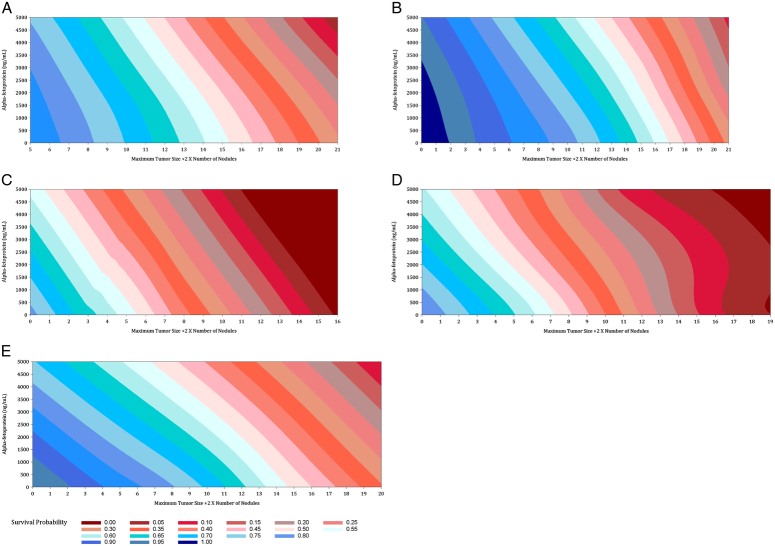
Surgical resection is a curative therapy for early-stage hepatocellular carcinoma (HCC) patients meeting the Milan criteria as well as a widely used therapy in intermediate-stage HCC. However, intermediate-stage HCC encompasses a wide spectrum of disease and there is a lack of good predictive models for the long-term clinical outcome of HCC patients currently. Here, the authors adopt Mazzaferro's Metroticket 2.0 to create a robust survival prediction model for intermediate-stage HCC patients undergoing surgical resection. Our algorithm considers age, AFP levels, ALBI score, and nodule size/number to generate survival estimates in an accessible graph format. Importantly, their model surpasses the American Joint Committee on Cancer staging model and was validated with independent US patient data.
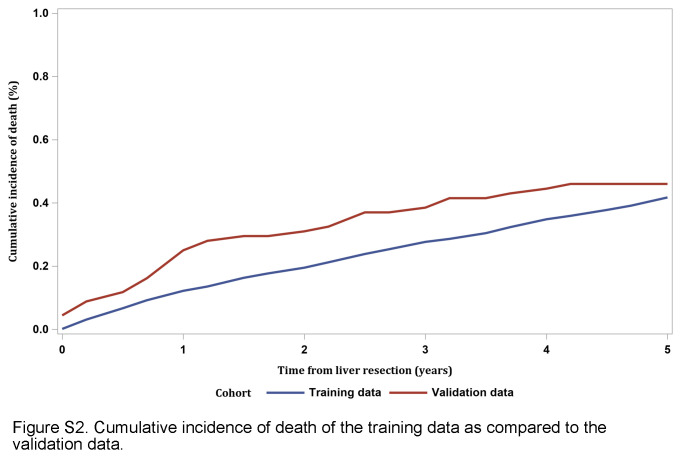
The authors conducted a retrospective analysis of OS and RFS in early- and intermediate-stage HCC patients treated with liver resection, including a training cohort in Singapore and a validation cohort in North Carolina, USA.
The authors recorded 278 deaths (35.0%) and 428 patients (53.9%) in the first 5 years after surgical resection; higher ALBI score, higher lnAFP, more advanced age and higher tumour burden index were identified as significant parameters. The overall predictive capability of our model, with the inclusion of AFP, is reflected with a UNO's C-statistic of 0.655, which is 1.11 times better than the 0.5895 C-statistic of the 8th AJCC TNM Staging model.
The authors' modified Metroticket model allows for more granular and better-informed prognostication. This will help surgeons and patients make accurate comparisons between the clinical outcomes of surgical resection and other non-surgical treatments.
手术切除是符合米兰标准的早期肝细胞癌(HCC)患者的一种治愈性疗法,也是中期HCC中广泛使用的疗法。然而,中期HCC涵盖了广泛的疾病范围,目前缺乏针对HCC患者长期临床结局的良好预测模型。在此,作者采用马扎法罗的Metroticket 2.0为接受手术切除的中期HCC患者创建一个强大的生存预测模型。我们的算法考虑年龄、甲胎蛋白(AFP)水平、白蛋白-胆红素(ALBI)评分和结节大小/数量,以可访问的图表形式生成生存估计值。重要的是,他们的模型超越了美国癌症联合委员会(AJCC)分期模型,并通过美国独立患者数据进行了验证。
作者对接受肝切除治疗的早期和中期HCC患者的总生存期(OS)和无复发生存期(RFS)进行了回顾性分析,包括新加坡的一个训练队列和美国北卡罗来纳州的一个验证队列。
作者记录了手术切除后前5年的278例死亡(35.0%)和428例患者(53.9%);较高的ALBI评分、较高的AFP对数、较高的年龄和较高的肿瘤负担指数被确定为显著参数。我们的模型(纳入AFP)的总体预测能力通过UNO的C统计量0.655体现,这比第8版AJCC TNM分期模型的0.5895 C统计量要好1.11倍。
作者改良的Metroticket模型能够进行更细致、信息更充分的预后评估。这将有助于外科医生和患者准确比较手术切除与其他非手术治疗的临床结局。