Hart Joseph P, Davies Mark G
Center for Quality, Effectiveness, and Outcomes in Cardiovascular Diseases, Houston, TX 77054, USA.
Division of Vascular and Endovascular Surgery, Medical College of Wisconsin, Milwaukee, WI 53226, USA.
J Clin Med. 2024 Aug 31;13(17):5170. doi: 10.3390/jcm13175170.
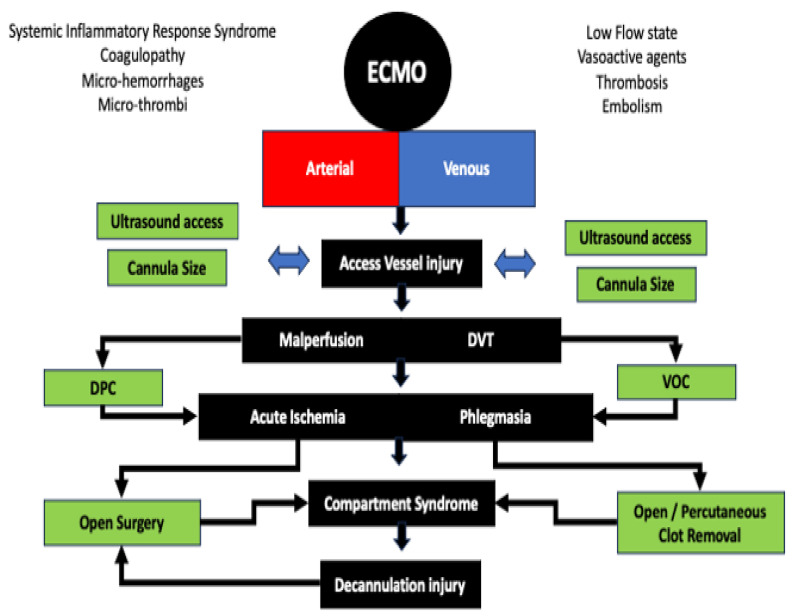
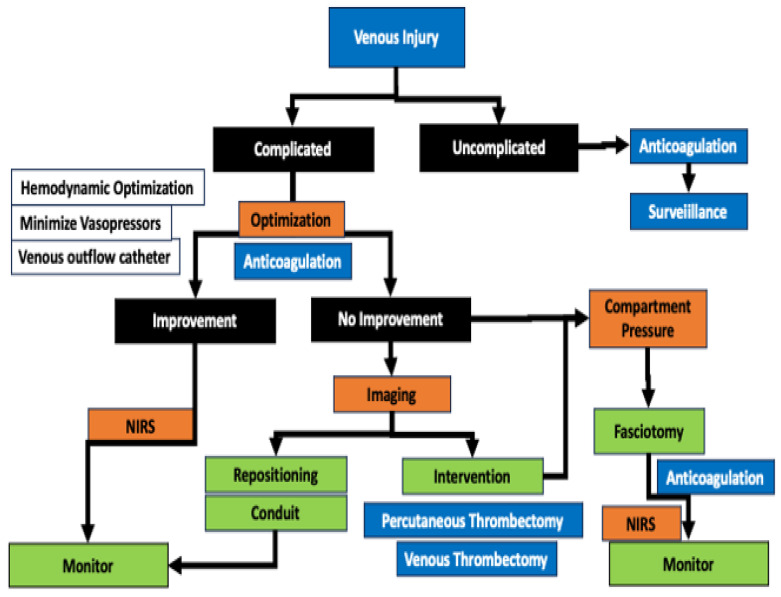
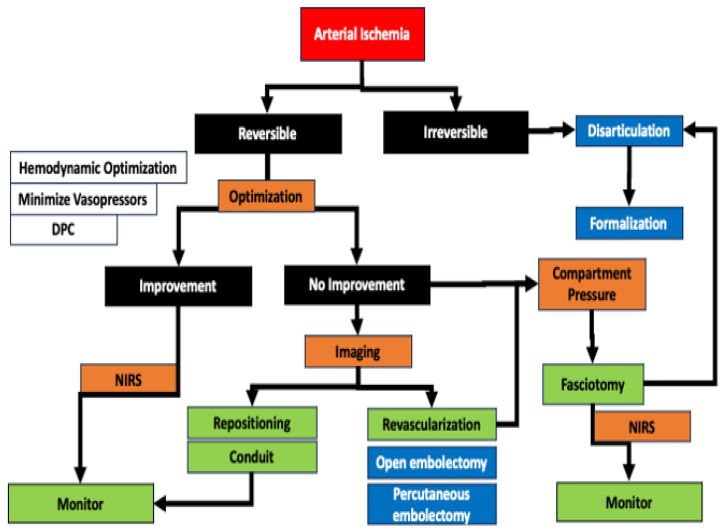
The establishment of a peripheral ECMO circuit can lead to significant arterial and venous complications in 10-30% of patients. Vascular complications, particularly acute limb ischemia, are associated with worsening overall outcomes. Limb ischemia occurs significantly more frequently in the early stages of VA ECMO than in VV ECMO. Mechanisms of limb ischemia include arterial obstruction, cannulation injury, loss of pulsatile flow, thromboembolism, venous stasis from compressive obstruction with large venous cannulas, and systemic vasoconstriction due to shock and pharmacologic vasoconstriction. The care team may use several mitigation strategies to prevent limb ischemia. Arterial and venous complications can be mitigated by careful access site selection, minimizing cannula size, placement of distal perfusion and/or outflow catheter(s), and continuous NIRS monitoring. Rapid intervention, when ischemia or compartment syndrome occurs, can reduce limb loss but may not affect the mortality and morbidity of the ECMO patient in the long term due to their underlying conditions and the etiology of the ECMO need.
建立外周体外膜肺氧合(ECMO)回路可导致10%-30%的患者出现严重的动脉和静脉并发症。血管并发症,尤其是急性肢体缺血,与总体预后恶化相关。肢体缺血在VA ECMO早期的发生频率明显高于VV ECMO。肢体缺血的机制包括动脉阻塞、插管损伤、搏动性血流丧失、血栓栓塞、大静脉插管压迫性阻塞导致的静脉淤滞,以及休克和药物性血管收缩引起的全身血管收缩。护理团队可采用多种缓解策略来预防肢体缺血。通过仔细选择穿刺部位、尽量减小插管尺寸、放置远端灌注和/或流出导管,以及持续近红外光谱(NIRS)监测,可减轻动脉和静脉并发症。当发生缺血或骨筋膜室综合征时,快速干预可减少肢体丢失,但由于ECMO患者的基础疾病和需要ECMO的病因,从长期来看可能不会影响其死亡率和发病率。