College of Medicine, Medical University of South Carolina, Charleston, SC, USA.
Surgical Service, Ralph H. Johnson Department of Veterans Affairs Medical Center, Charleston, SC, USA.
Langenbecks Arch Surg. 2024 Sep 17;409(1):280. doi: 10.1007/s00423-024-03470-1.
Blind tunneling of subfascial femoropopliteal bypass grafts may result in inadvertent graft passage through the sartorius. The purpose of this study was to determine whether intramuscular passage of femoropopliteal bypass grafts affects primary patency.
Patients undergoing femoropopliteal bypass at a Veterans Administration hospital and associated university medical center over a recent 13-year period who also had postoperative cross-sectional imaging adequate to determine graft location were examined. Five-year primary patency of grafts circumferentially enveloped by the muscle was compared with that of both extramuscular subfascial grafts and subcutaneous grafts.
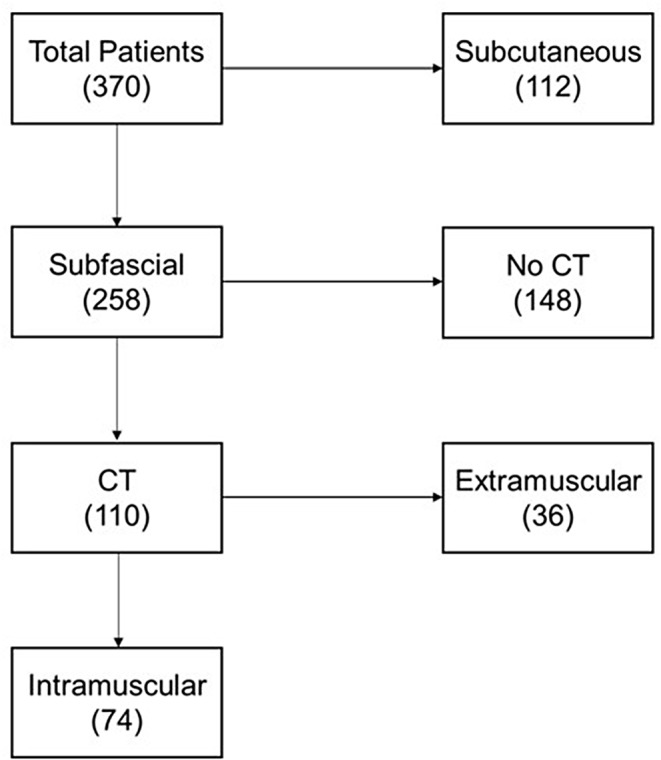
370 femoropopliteal grafts were identified, among which 258 (70%) were subfascial. Vein grafts comprised 51% of the subfascial grafts, and 53% were inserted above the knee. Available postoperative imaging in 110 subfascial grafts demonstrated 74 (67%) to lie completely within the muscle at some point. Among imaged subfascial grafts, primary patency at five years for intramuscular grafts was not significantly worse than extramuscular grafts (P = 0.31). This remained true whether grafts were vein (P = 0.39) or prosthetic (P = 0.31) and whether grafts inserted to the above-knee (P = 0.43) or below-knee (P = 0.21) popliteal artery. Multivariable Cox regression revealed a significant relationship between use of vein grafts (P = 0.013), active smoking (P = 0.01), and hypertension (P = 0.041) and primary patency, but not intramuscular graft location (P = 0.31).
This study failed to demonstrate significantly inferior primary patency among subfascial femoropopliteal grafts tunneled intramuscularly. Larger studies may be required to adequately detect any differences in patency by muscular entrapment, especially among subgroups.
股腘旁路移植的皮下盲目隧道可能导致移植无意中穿过缝匠肌。本研究的目的是确定股腘旁路移植的肌内通过是否会影响原发性通畅率。
在最近的 13 年期间,在退伍军人事务医院和相关大学医疗中心进行股腘旁路手术的患者,并且术后有足够的横断面成像来确定移植物位置,对这些患者进行了检查。比较了被肌肉环绕的移植的 5 年原发性通畅率与皮下和皮下的移植物。
确定了 370 例股腘旁路移植,其中 258 例(70%)为皮下。静脉移植物占皮下移植物的 51%,53%位于膝关节以上。110 例皮下移植物的术后影像学显示,74 例(67%)在某一点完全位于肌肉内。在成像的皮下移植物中,肌内移植物的 5 年原发性通畅率与非肌内移植物无显著差异(P = 0.31)。这一结果在静脉移植物(P = 0.39)或假体移植物(P = 0.31)、膝关节以上(P = 0.43)或膝关节以下(P = 0.21)的腘动脉插入的移植物中均成立。多变量 Cox 回归显示,静脉移植物的使用(P = 0.013)、吸烟(P = 0.01)和高血压(P = 0.041)与原发性通畅率有显著关系,但与肌内移植物位置无关(P = 0.31)。
本研究未能证明肌内隧道的皮下股腘旁路移植物的原发性通畅率明显降低。可能需要更大的研究来充分检测肌肉嵌塞对通畅率的任何差异,尤其是在亚组中。