Department of Pathology, Advanced Medical Research Institute Hospital, Kolkata, India.
Department of Pathology, Core Diagnostics, Gurgaon, India.
Virchows Arch. 2024 Nov;485(5):829-840. doi: 10.1007/s00428-024-03909-2. Epub 2024 Sep 17.
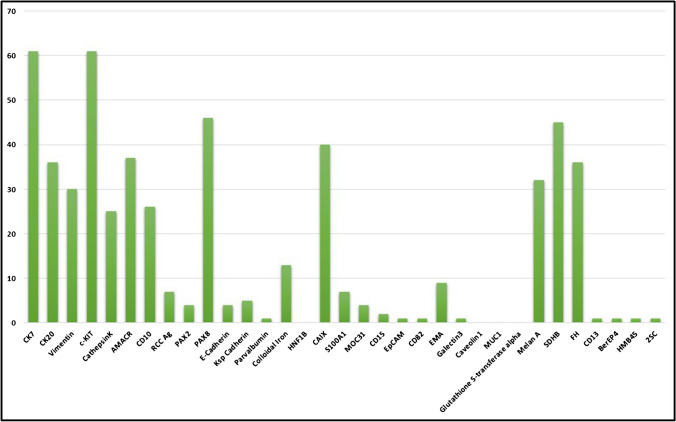
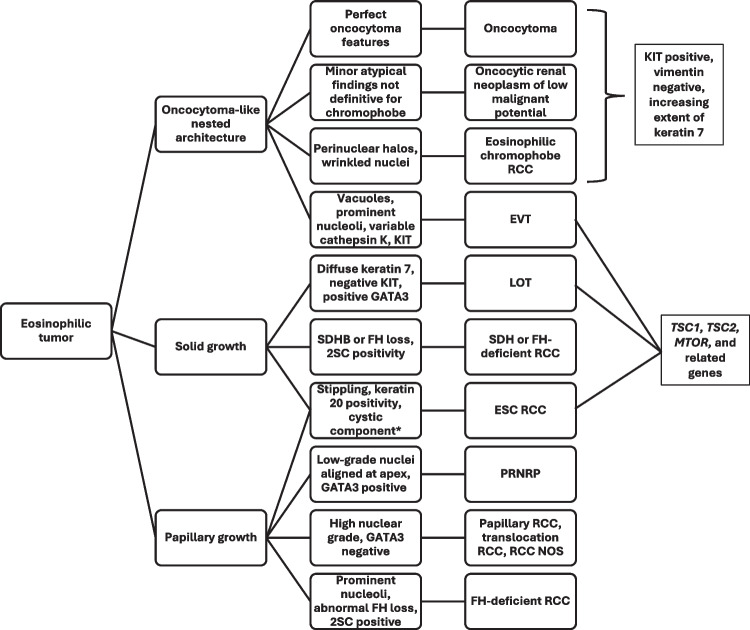
Oncocytic renal neoplasms are a major source of diagnostic challenge in genitourinary pathology; however, they are typically nonaggressive in general, raising the question of whether distinguishing different subtypes, including emerging entities, is necessary. Emerging entities recently described include eosinophilic solid and cystic renal cell carcinoma (ESC RCC), low-grade oncocytic tumor (LOT), eosinophilic vacuolated tumor (EVT), and papillary renal neoplasm with reverse polarity (PRNRP). A survey was shared among 65 urologic pathologists using SurveyMonkey.com (Survey Monkey, Santa Clara, CA, USA). De-identified and anonymized respondent data were analyzed. Sixty-three participants completed the survey and contributed to the study. Participants were from Asia (n = 21; 35%), North America (n = 31; 52%), Europe (n = 6; 10%), and Australia (n = 2; 3%). Half encounter oncocytic renal neoplasms that are difficult to classify monthly or more frequently. Most (70%) indicated that there is enough evidence to consider ESC RCC as a distinct entity now, whereas there was less certainty for LOT (27%), EVT (29%), and PRNRP (37%). However, when combining the responses for sufficient evidence currently and likely in the future, LOT and EVT yielded > 70% and > 60% for PRNRP. Most (60%) would not render an outright diagnosis of oncocytoma on needle core biopsy. There was a dichotomy in the routine use of immunohistochemistry (IHC) in the evaluation of oncocytoma (yes = 52%; no = 48%). The most utilized IHC markers included keratin 7 and 20, KIT, AMACR, PAX8, CA9, melan A, succinate dehydrogenase (SDH)B, and fumarate hydratase (FH). Genetic techniques used included TSC1/TSC2/MTOR (67%) or TFE3 (74%) genes and pathways; however, the majority reported using these very rarely. Only 40% have encountered low-grade oncocytic renal neoplasms that are deficient for FH. Increasing experience with the spectrum of oncocytic renal neoplasms will likely yield further insights into the most appropriate work-up, classification, and clinical management for these entities.
Oncocytic 肾肿瘤是泌尿生殖系统病理学中主要的诊断挑战来源;然而,它们通常总体上侵袭性较低,这就提出了一个问题,即是否需要区分不同的亚型,包括新出现的实体。最近描述的新实体包括嗜酸细胞实性和囊性肾细胞癌 (ESC RCC)、低级别嗜酸细胞瘤 (LOT)、嗜酸细胞空泡性肿瘤 (EVT) 和具有反向极性的乳头状肾肿瘤 (PRNRP)。一项调查通过 SurveyMonkey.com(Survey Monkey,美国加利福尼亚州圣克拉拉)在 65 位泌尿科病理学家中进行。对匿名和匿名的应答者数据进行了分析。63 名参与者完成了调查并为研究做出了贡献。参与者来自亚洲 (n=21;35%)、北美 (n=31;52%)、欧洲 (n=6;10%) 和澳大利亚 (n=2;3%)。一半的人每月或更频繁地遇到难以分类的嗜酸细胞肾肿瘤。大多数人 (70%) 表示,现在有足够的证据将 ESC RCC 视为一个独特的实体,而 LOT (27%)、EVT (29%) 和 PRNRP (37%) 的确定性较低。然而,当结合目前和未来可能有足够证据的反应时,LOT 和 EVT 的反应率均超过 70%,PRNRP 的反应率超过 60%。大多数人 (60%) 不会在针芯活检中直接诊断为嗜酸细胞瘤。在评估嗜酸细胞瘤时,免疫组织化学 (IHC) 的常规使用存在二分法 (是=52%;否=48%)。最常用的 IHC 标志物包括角蛋白 7 和 20、KIT、AMACR、PAX8、CA9、黑色素 A、琥珀酸脱氢酶 (SDHB) 和延胡索酸水合酶 (FH)。使用的遗传技术包括 TSC1/TSC2/MTOR (67%) 或 TFE3 (74%) 基因和途径;然而,大多数人报告很少使用这些技术。只有 40% 的人遇到 FH 缺乏的低级别嗜酸细胞瘤。随着对嗜酸细胞瘤肾肿瘤谱的经验不断增加,可能会进一步深入了解这些实体最适当的检查、分类和临床管理。