Tangsermvong Poonyisa, Chamroonrat Wichana, Vittayachokkitikhun Siripong, Sriphrapradang Chutintorn
Department of Medicine, Faculty of Medicine Ramathibodi hospital, Mahidol University, Bangkok, Thailand.
Division of Nuclear Medicine, Department of Radiology, Faculty of Medicine Ramathibodi hospital, Mahidol University, Bangkok, Thailand.
Clin Med Insights Endocrinol Diabetes. 2024 Sep 10;17:11795514241278519. doi: 10.1177/11795514241278519. eCollection 2024.
Several case reports and a few studies have reported that hypothyroid patients have elevated serum potassium levels. However, hypothyroidism has not been widely accepted as a cause of hyperkalemia.
This study aims to evaluate the incidence of hyperkalemia and factors influencing serum potassium levels in thyroid cancer patients with hypothyroidism during thyroid hormone withdrawal before radioactive iodine (RAI) treatment.
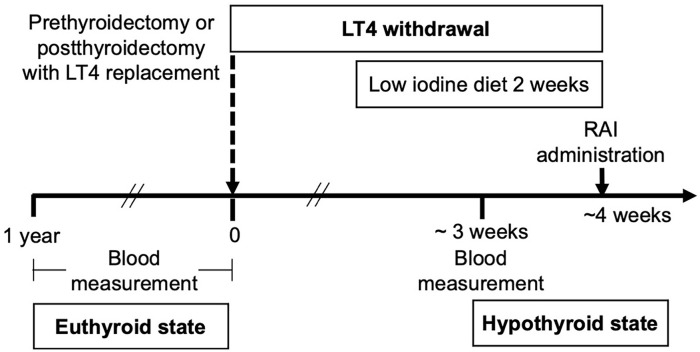
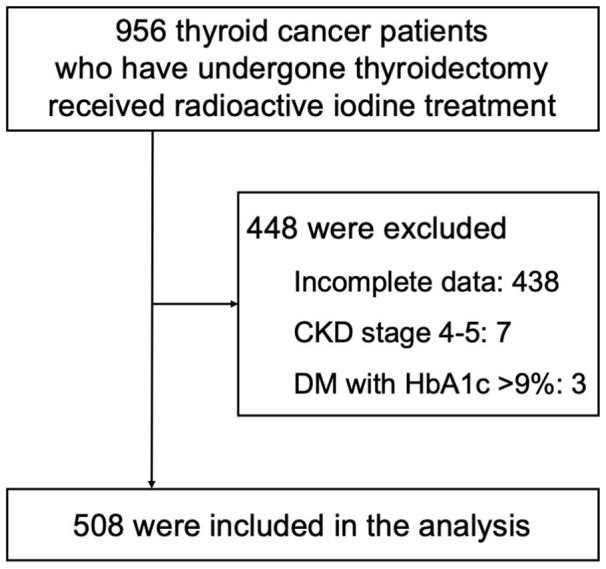
We conducted a retrospective review of electronic medical records from January 2017 to June 2021, involving 956 thyroid cancer patients post-thyroidectomy and undergoing RAI. Laboratory parameters, including serum potassium levels, were collected in both euthyroid (<1 year prior to RAI) and hypothyroid states.
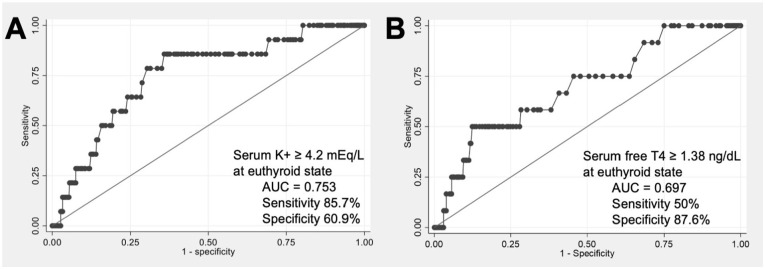
Among 508 patients (mean age 52 years, 79.3% female), hyperkalemia (potassium ⩾ 5.0 mEq/L) occurred in 2.8%, without severe hyperkalemia (potassium ⩾ 6.5 mEq/L). The hypothyroid state exhibited significantly higher serum potassium than the euthyroid state [4.16 (IQR, 3.94-4.41) vs 4.10 (IQR, 3.90-4.35) mEq/L, < .01]. The mean change in potassium levels between the euthyroid and hypothyroid state was 0.05 ± 0.17 mEq/L. Pre-thyroid hormone withdrawal (euthyroid state) factors associated with serum potassium levels in the hypothyroid state included age, use of angiotensin-converting enzyme inhibitors, diabetes mellitus, serum BUN/creatinine, serum potassium levels, hemoglobin A1c (positive correlation); and thiazide use and eGFR (negative correlation). In the hypothyroid state, hyperkalemia was more likely in patients with serum potassium ⩾4.2 mEq/L (OR 9.36, < .01) or free T4 ⩾1.38 ng/dL (OR 7.05, < .01) during the euthyroid state.
The incidence of hyperkalemia was low in our hypothyroid cohorts. However, physicians should remain vigilant for cases with risk factors for developing hyperkalemia.
多项病例报告和一些研究报道甲状腺功能减退患者血清钾水平升高。然而,甲状腺功能减退作为高钾血症的病因尚未被广泛接受。
本研究旨在评估甲状腺癌伴甲状腺功能减退患者在放射性碘(RAI)治疗前甲状腺激素撤减期间高钾血症的发生率及影响血清钾水平的因素。
我们对2017年1月至2021年6月的电子病历进行了回顾性分析,纳入956例行甲状腺切除术后接受RAI治疗的甲状腺癌患者。收集甲状腺功能正常(RAI治疗前<1年)和甲状腺功能减退状态下的实验室参数,包括血清钾水平。
在508例患者(平均年龄52岁,女性占79.3%)中,高钾血症(血钾⩾5.0 mEq/L)发生率为2.8%,无严重高钾血症(血钾⩾6.5 mEq/L)。甲状腺功能减退状态下的血清钾水平显著高于甲状腺功能正常状态[4.16(四分位间距,3.94 - 4.41) vs 4.10(四分位间距,3.90 - 4.35)mEq/L,P <.01]。甲状腺功能正常和减退状态之间钾水平的平均变化为0.05±0.17 mEq/L。甲状腺激素撤减前(甲状腺功能正常状态)与甲状腺功能减退状态下血清钾水平相关的因素包括年龄、血管紧张素转换酶抑制剂的使用、糖尿病、血清尿素氮/肌酐、血清钾水平、糖化血红蛋白(正相关);以及噻嗪类药物的使用和估算肾小球滤过率(负相关)。在甲状腺功能减退状态下,甲状腺功能正常时血钾⩾4.2 mEq/L(比值比9.36,P <.01)或游离T4⩾1.38 ng/dL(比值比7.05,P <.01)的患者更易发生高钾血症。
我们的甲状腺功能减退队列中高钾血症发生率较低。然而,医生应对有高钾血症发生风险因素的病例保持警惕。