Department of Haematology, St. George and Sutherland Clinical Campuses, School of Clinical Medicine, Faculty of Medicine and Health, University of New South Wales, Sydney, NSW, Australia.
Biological Resources Imaging Laboratory, Mark Wainwright Analytical Centre, University of New South Wales, Sydney, NSW, Australia.
Blood Adv. 2024 Nov 26;8(22):5744-5752. doi: 10.1182/bloodadvances.2024013883.
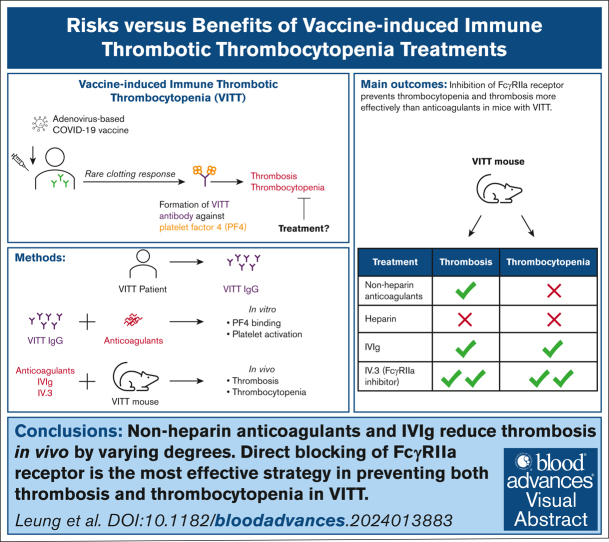
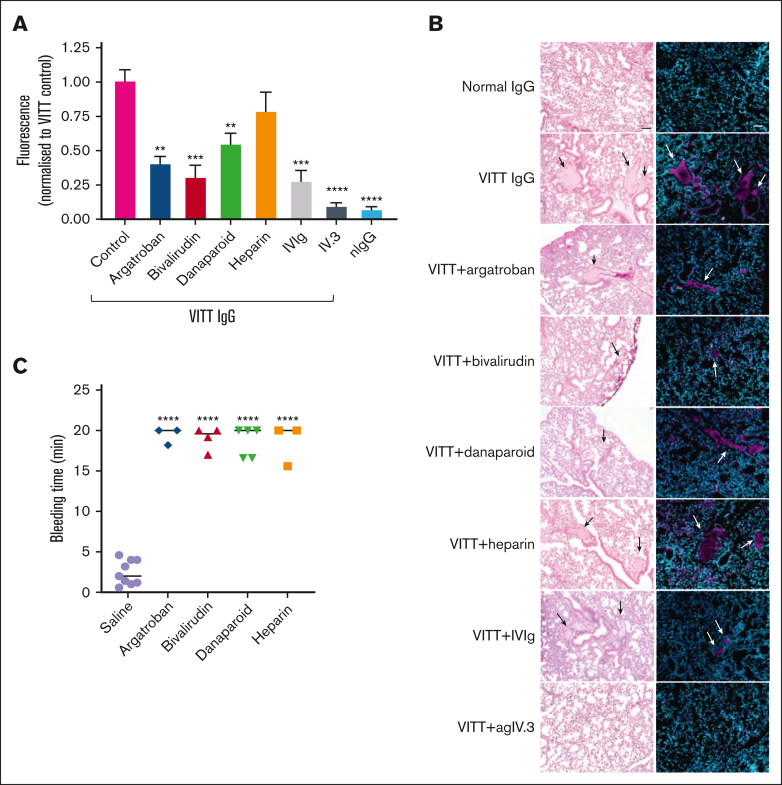
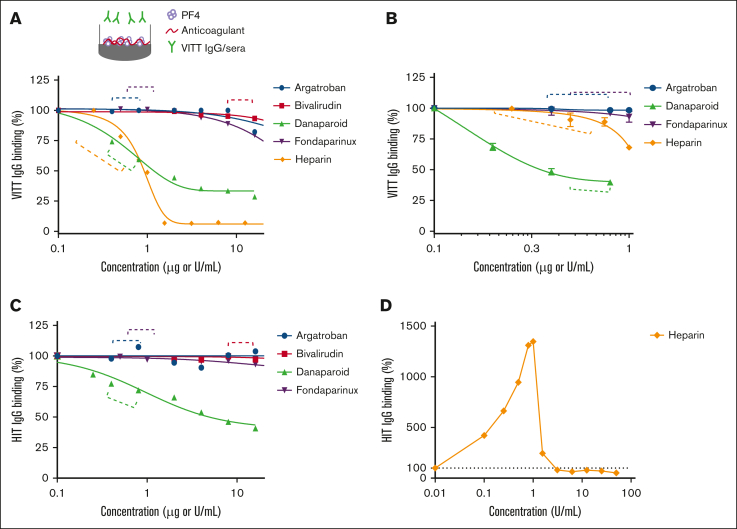
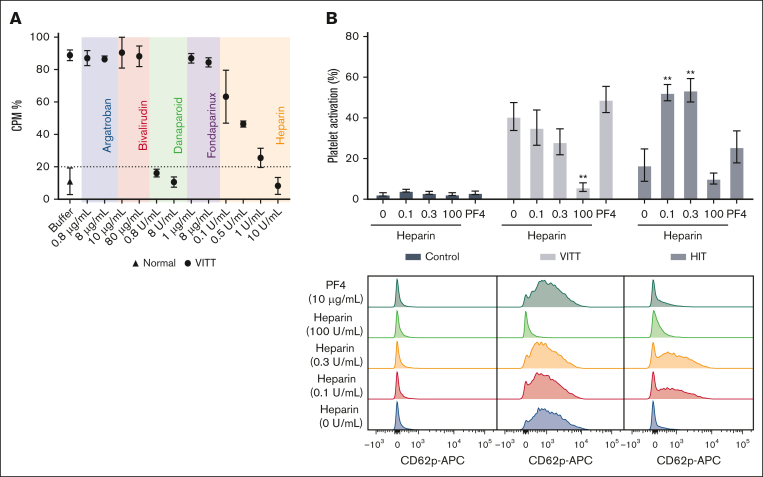
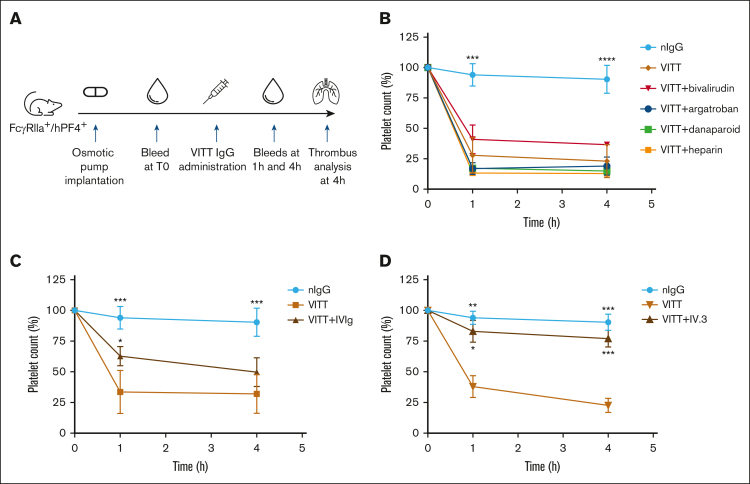
Current guidelines for treating vaccine-induced immune thrombotic thrombocytopenia (VITT) recommend nonheparin anticoagulants and IV immunoglobulin (IVIg). However, the efficacy of these treatments remains uncertain due to case studies involving small patient numbers, confounding factors (eg, concurrent treatments), and a lack of animal studies. A recent study proposed danaparoid and heparin as potential VITT therapies because of their ability to disrupt VITT IgG-platelet factor 4 (PF4) binding. Here, we examined the effects of various anticoagulants (including unfractionated [UF] heparin, danaparoid, bivalirudin, fondaparinux, and argatroban), IVIg, and the FcγRIIa receptor-blocking antibody, IV.3. Our investigation focused on VITT IgG-PF4 binding, platelet activation, thrombocytopenia, and thrombosis. Danaparoid, at therapeutic doses, was the sole anticoagulant that reduced VITT IgG-PF4 binding, verified by affinity-purified anti-PF4 VITT IgG. Although danaparoid and high-dose UF heparin (10 U/mL) inhibited platelet activation, none of the anticoagulants significantly affected thrombocytopenia in our VITT animal model and all prolonged bleeding time. IVIg and all anticoagulants except UF heparin protected the VITT mice from thrombosis. Direct FcγRIIa receptor inhibition with IV.3 antibody is an effective approach for managing both thrombosis and thrombocytopenia in the VITT mouse model. Our results underscore the necessity of animal model investigations to inform and better guide clinicians on treatment choices. This study provides compelling evidence for the development of FcγRIIa receptor blockers to prevent thrombosis in VITT and other FcγRIIa-related inflammatory disorders.
目前治疗疫苗诱导的免疫性血栓性血小板减少症(VITT)的指南建议使用非肝素抗凝剂和静脉注射免疫球蛋白(IVIg)。然而,由于涉及患者数量较少、混杂因素(如同时进行的治疗)以及缺乏动物研究,这些治疗方法的疗效仍不确定。最近的一项研究提出达那肝素和肝素可能是 VITT 的潜在治疗方法,因为它们能够破坏 VITT IgG-血小板因子 4(PF4)结合。在这里,我们研究了各种抗凝剂(包括未分级肝素、达那肝素、比伐卢定、磺达肝癸钠和阿加曲班)、IVIg 和 FcγRIIa 受体阻断抗体 IV.3 的作用。我们的研究重点是 VITT IgG-PF4 结合、血小板活化、血小板减少症和血栓形成。达那肝素在治疗剂量下是唯一能降低 VITT IgG-PF4 结合的抗凝剂,这通过亲和纯化的抗 PF4 VITT IgG 得到了验证。尽管达那肝素和高剂量未分级肝素(10 U/mL)抑制了血小板活化,但在我们的 VITT 动物模型中,没有一种抗凝剂能显著影响血小板减少症,所有抗凝剂都延长了出血时间。IVIg 和除未分级肝素以外的所有抗凝剂都能保护 VITT 小鼠免受血栓形成。用 IV.3 抗体直接抑制 FcγRIIa 受体是一种有效的方法,可以治疗 VITT 小鼠模型中的血栓形成和血小板减少症。我们的结果强调了动物模型研究的必要性,以便为临床医生提供治疗选择的信息并更好地指导他们。这项研究为开发 FcγRIIa 受体抑制剂以预防 VITT 和其他 FcγRIIa 相关炎症性疾病中的血栓形成提供了有力证据。