Department of Global Health and Development, London School of Hygiene and Tropical Medicine, London, United Kingdom.
Department of Psychiatric Social Work, National Institue of Mental Health and Neurosciences, Bangalore, India.
Health Res Policy Syst. 2024 Sep 18;22(1):127. doi: 10.1186/s12961-024-01184-w.
The importance of evidence-informed health policymaking is widely recognized. However, many low- and middle-income countries lack evidence-informed mental health policies due to insufficient data, stigma or lack of resources. Various policies address adolescent mental health in India, but published knowledge on their evidence-informed nature is limited. In this paper, we report results of our analysis of the role of evidence in adolescent mental health policymaking in India.
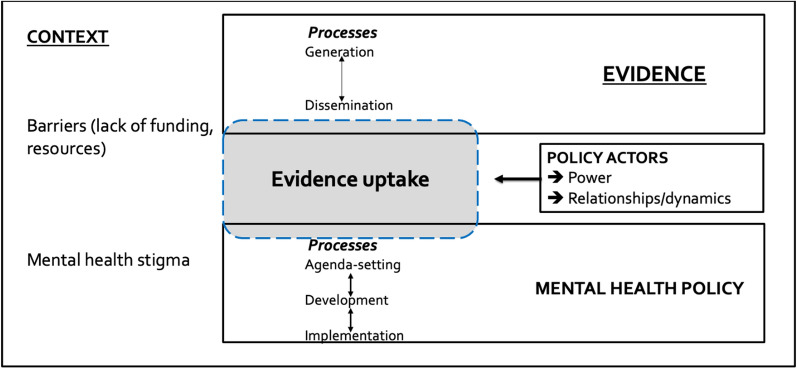
This paper reports findings from the document analysis of key policy documentation (n = 10) and in-depth interviews with policy actors including policymakers, researchers, practitioners and intermediaries (n = 13). Framework analysis was used, informed by the components of a conceptual framework adapted from the literature: actors, policy and evidence processes, nature of evidence itself and contextual influences.
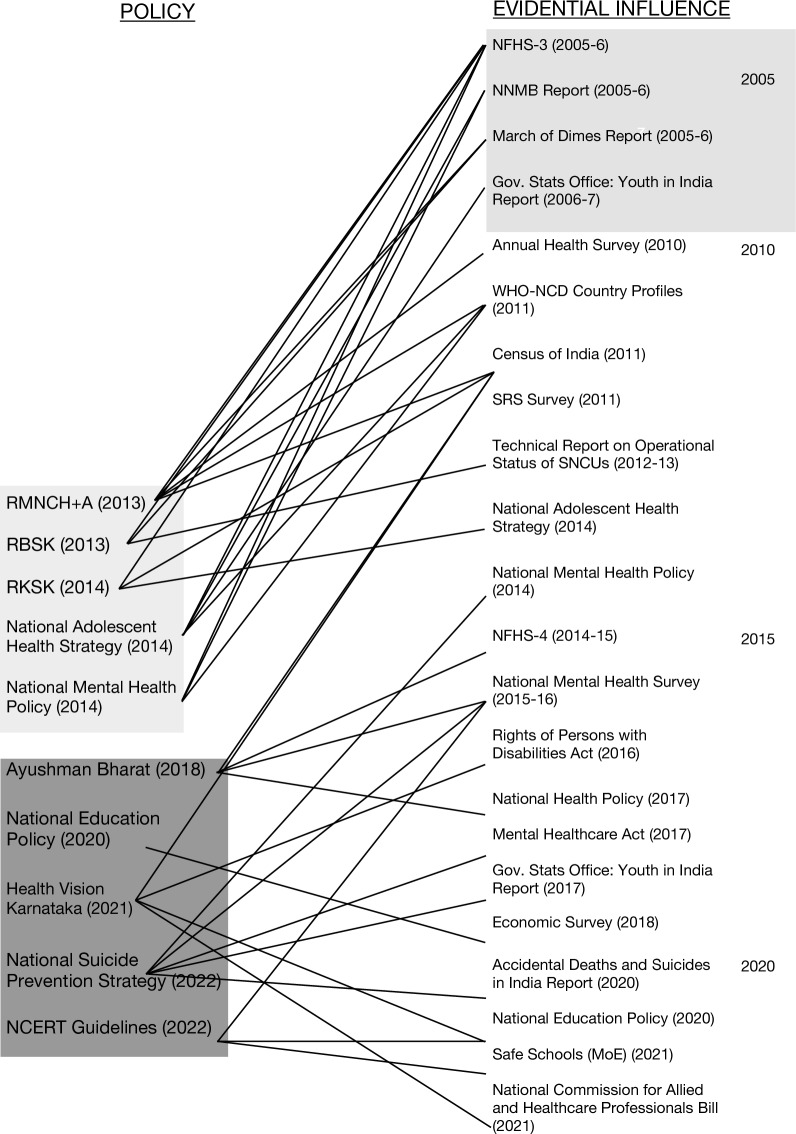
Results show that adolescent mental health policies in India were generally evidence-informed, with more key evidence becoming generally available from 2010 onwards. Both formal and informal evidence informed mental health policies, particularly agenda-setting and policy development. Mental health policymaking in India is deemed important yet relatively neglected due to competing policy priorities and structural barriers such as stigma. Use of evidence in mental health policymaking reflected differing values, interests, relative powers and ideologies of policy actors. Involvement of government officials in evidence generation often resulted in successful evidence uptake in policy decisions. Policy actors often favoured formal and quantitative evidence, with a tendency to accept global evidence that aligns with personal values.
There is a need to ensure a balanced and complementary combination of formal and informal evidence for policy decisions. Evidence generation, dissemination and use for policy processes should recognize evidence preferences by key stakeholders, while prioritizing locally available evidence where possible. To help this, a balanced involvement of policy actors can ensure complementary perspectives in evidence production and policy agendas. This continued generation and promotion of evidence can also help reduce societal stigma around mental health and promote mental health as a key policy priority.
循证卫生决策的重要性已得到广泛认可。然而,许多低收入和中等收入国家由于数据不足、污名化或缺乏资源,缺乏循证精神卫生政策。印度有各种政策涉及青少年心理健康问题,但发表的关于其循证性质的知识有限。在本文中,我们报告了我们对印度青少年心理健康政策制定中证据作用的分析结果。
本文报告了对关键政策文件(n=10)进行文件分析和对政策制定者、研究人员、从业人员和中介机构(n=13)进行深入访谈的结果。使用框架分析,框架分析的依据是文献改编的概念框架的组成部分:行为者、政策和证据过程、证据本身的性质和背景影响。
结果表明,印度的青少年心理健康政策总体上是循证的,自 2010 年以来,更多的关键证据普遍可用。正式和非正式证据都为心理健康政策提供了信息,特别是为议程设定和政策制定提供了信息。印度的精神卫生政策制定虽然被认为很重要,但由于竞争的政策优先事项和结构性障碍,如污名化,相对被忽视。政策制定者在精神卫生政策制定中使用证据反映了不同的价值观、利益、相对权力和意识形态。政府官员参与证据的产生往往会导致在政策决策中成功地采用证据。政策制定者往往倾向于正式和定量的证据,并倾向于接受与个人价值观一致的全球证据。
需要确保政策决策中正式和非正式证据的平衡和互补结合。证据的生成、传播和使用应认识到主要利益相关者的证据偏好,同时在可能的情况下优先考虑当地可获得的证据。为了做到这一点,政策制定者的平衡参与可以确保在证据制作和政策议程方面具有互补性观点。这种持续的证据生成和推广也有助于减少社会对精神健康的污名化,促进精神健康成为一个关键的政策优先事项。