Stone Gregg W, Lindenfeld JoAnn, Rodés-Cabau Josep, Anker Stefan D, Zile Michael R, Kar Saibal, Holcomb Richard, Pfeiffer Michael P, Bayes-Genis Antoni, Bax Jeroen J, Bank Alan J, Costanzo Maria Rosa, Verheye Stefan, Roguin Ariel, Filippatos Gerasimos, Núñez Julio, Lee Elizabeth C, Laufer-Perl Michal, Moravsky Gil, Litwin Sheldon E, Prihadi Edgard, Gada Hemal, Chung Eugene S, Price Matthew J, Thohan Vinay, Schewel Dimitry, Kumar Sachin, Kische Stephan, Shah Kevin S, Donovan Daniel J, Zhang Yiran, Eigler Neal L, Abraham William T
The Zena and Michael A. Wiener Cardiovascular Institute, Icahn School of Medicine at Mount Sinai, New York, NY (G.W.S.).
Advanced Heart Failure, Vanderbilt Heart and Vascular Institute, Nashville, TN (J.L.).
Circulation. 2024 Dec 10;150(24):1931-1943. doi: 10.1161/CIRCULATIONAHA.124.070870. Epub 2024 Sep 23.
An interatrial shunt may provide an autoregulatory mechanism to decrease left atrial pressure and improve heart failure (HF) symptoms and prognosis.
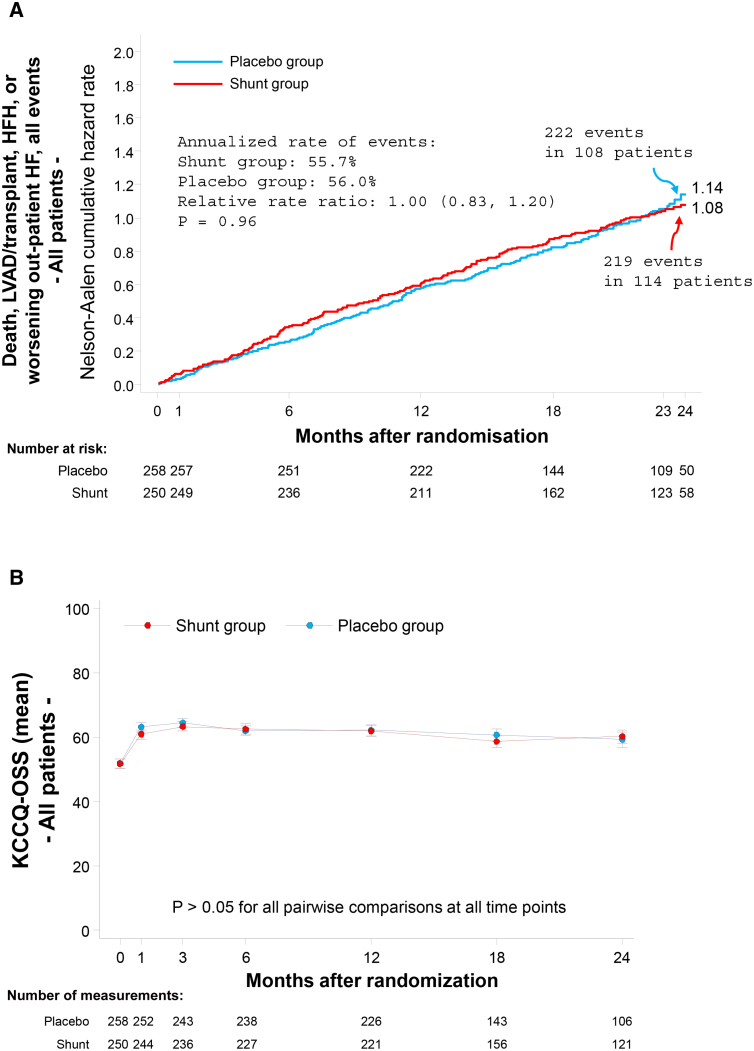
Patients with symptomatic HF with any left ventricular ejection fraction (LVEF) were randomized 1:1 to transcatheter shunt implantation versus a placebo procedure, stratified by reduced (≤40%) versus preserved (>40%) LVEF. The primary safety outcome was a composite of device-related or procedure-related major adverse cardiovascular or neurological events at 30 days compared with a prespecified performance goal of 11%. The primary effectiveness outcome was the hierarchical composite ranking of all-cause death, cardiac transplantation or left ventricular assist device implantation, HF hospitalization, outpatient worsening HF events, and change in quality of life from baseline measured by the Kansas City Cardiomyopathy Questionnaire overall summary score through maximum 2-year follow-up, assessed when the last enrolled patient reached 1-year follow-up, expressed as the win ratio. Prespecified hypothesis-generating analyses were performed in patients with reduced and preserved LVEF.
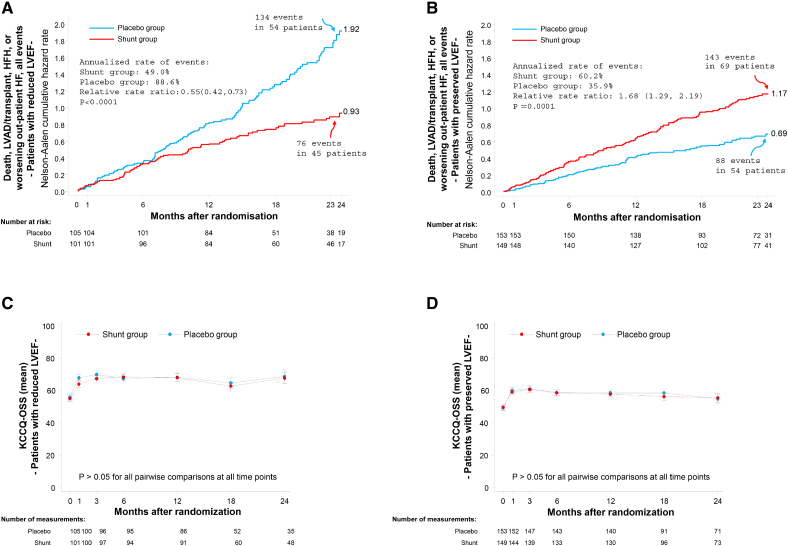
Between October 24, 2018, and October 19, 2022, 508 patients were randomized at 94 sites in 11 countries to interatrial shunt treatment (n=250) or a placebo procedure (n=258). Median (25th and 75th percentiles) age was 73.0 years (66.0, 79.0), and 189 patients (37.2%) were women. Median LVEF was reduced (≤40%) in 206 patients (40.6%) and preserved (>40%) in 302 patients (59.4%). No primary safety events occurred after shunt implantation (upper 97.5% confidence limit, 1.5%; <0.0001). There was no difference in the 2-year primary effectiveness outcome between the shunt and placebo procedure groups (win ratio, 0.86 [95% CI, 0.61-1.22]; =0.20). However, patients with reduced LVEF had fewer adverse cardiovascular events with shunt treatment versus placebo (annualized rate 49.0% versus 88.6%; relative risk, 0.55 [95% CI, 0.42-0.73]; <0.0001), whereas patients with preserved LVEF had more cardiovascular events with shunt treatment (annualized rate 60.2% versus 35.9%; relative risk, 1.68 [95% CI, 1.29-2.19]; =0.0001; <0.0001). There were no between-group differences in change in Kansas City Cardiomyopathy Questionnaire overall summary score during follow-up in all patients or in those with reduced or preserved LVEF.
Transcatheter interatrial shunt implantation was safe but did not improve outcomes in patients with HF. However, the results from a prespecified exploratory analysis in stratified randomized groups suggest that shunt implantation is beneficial in patients with reduced LVEF and harmful in patients with preserved LVEF.
URL: https://www.clinicaltrials.gov; Unique identifier: NCT03499236.
房间隔分流术可能提供一种自动调节机制,以降低左心房压力,改善心力衰竭(HF)症状和预后。
有症状的HF患者,无论左心室射血分数(LVEF)如何,均按1:1随机分为经导管分流植入组和安慰剂组,按LVEF降低(≤40%)与保留(>40%)分层。主要安全结局是30天时与预设的11%的性能目标相比,与器械相关或手术相关的主要不良心血管或神经系统事件的复合结局。主要有效性结局是全因死亡、心脏移植或左心室辅助装置植入、HF住院、门诊HF恶化事件以及通过堪萨斯城心肌病问卷总体总结评分从基线测量的生活质量变化的分层复合排名,随访最长2年,在最后一名入组患者达到1年随访时进行评估,以胜率表示。对LVEF降低和保留的患者进行了预设的假设生成分析。
在2018年10月24日至2022年10月19日期间,11个国家94个地点的508例患者被随机分为房间隔分流治疗组(n = 250)或安慰剂组(n = 258)。年龄中位数(第25和第75百分位数)为73.0岁(66.0,79.0),189例患者(37.2%)为女性。206例患者(40.6%)的LVEF中位数降低(≤40%),302例患者(59.4%)的LVEF保留(>40%)。分流植入后未发生主要安全事件(97.5%置信上限,1.5%;<0.0001)。分流组和安慰剂组在2年主要有效性结局方面无差异(胜率,0.86 [95% CI,0.61 - 1.22];P = 0.20)。然而,LVEF降低的患者与安慰剂相比,分流治疗的不良心血管事件更少(年化率49.0%对88.6%;相对风险,0.55 [95% CI,0.42 - 0.73];<0.0001),而LVEF保留的患者分流治疗的心血管事件更多(年化率60.2%对35.9%;相对风险,1.68 [95% CI,1.29 - 2.19];P = 0.0001;<0.0001)。在所有患者或LVEF降低或保留的患者随访期间,堪萨斯城心肌病问卷总体总结评分的变化在组间无差异。
经导管房间隔分流植入术是安全的,但未改善HF患者的结局。然而,分层随机分组中预设的探索性分析结果表明,分流植入对LVEF降低的患者有益,对LVEF保留的患者有害。