Lacaita Pietro G, Kindl Benedikt, Plank Fabian, Beyer Christoph, Bilgeri Valentin, Barbieri Fabian, Senoner Thomas, Dichtl Wolfgang, Tancevski Ivan, Swoboda Michael, Luger Anna, Deeg Johannes, Widmann Gerlig, Feuchtner Gudrun M
Department of Radiology, Innsbruck Medical University, Innsbruck, Austria.
Department of Internal Medicine, Tyrol Clinicum Hall, Hall, Austria.
ERJ Open Res. 2024 Sep 23;10(5). doi: 10.1183/23120541.00295-2024. eCollection 2024 Sep.
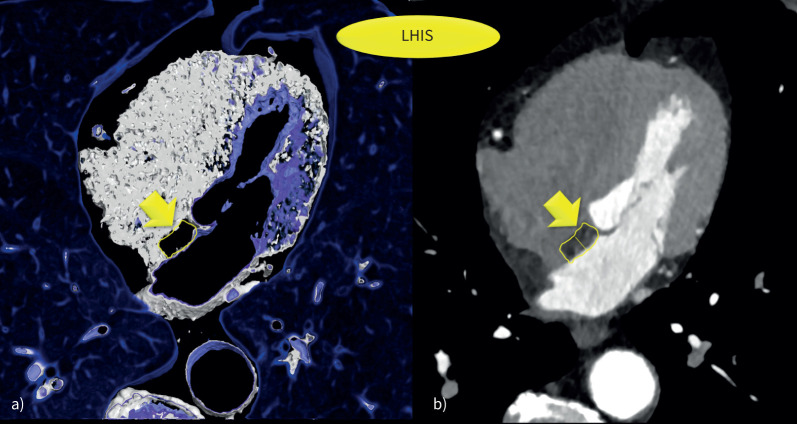
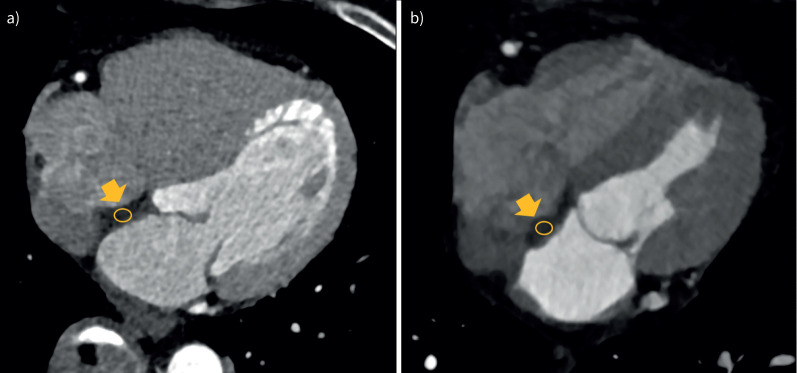
Lipomatous hypertrophy of the interatrial septum (LHIS) is a distinct section of epicardial adipose tissue. However, its association with COPD is poorly documented.
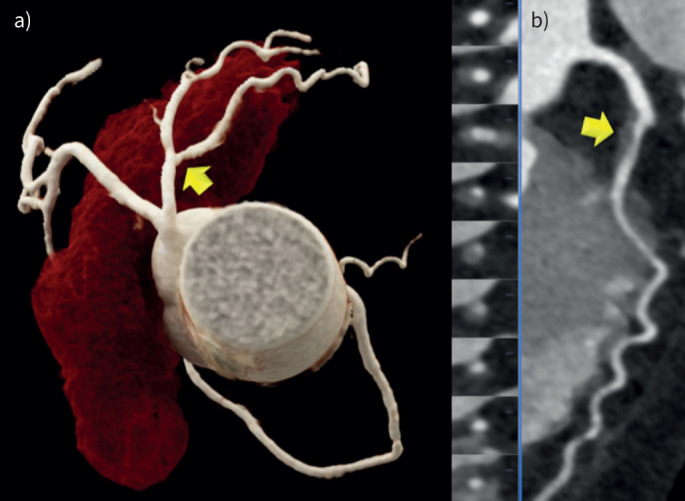
Patients undergoing coronary computed tomography angiography (CTA) for clinical indications were recruited retrospectively and screened for LHIS and COPD. LHIS density and the coronary artery disease profile were quantified by CTA: stenosis severity (coronary artery disease radiological reporting system (CADRADS)), coronary artery calcium (CAC) and high-risk plaque (HRP). COPD patients with LHIS were matched for age and sex, the major cardiovascular risk factors (CVRFs), and compared to controls.
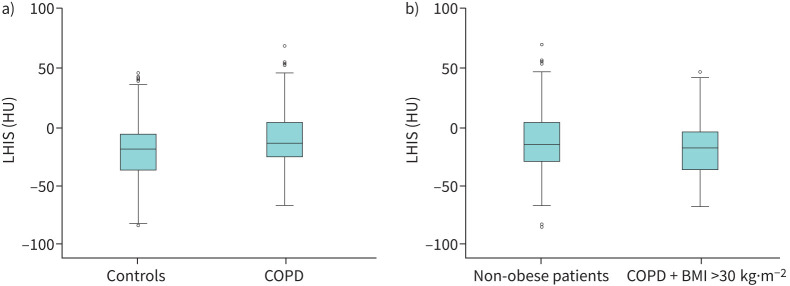
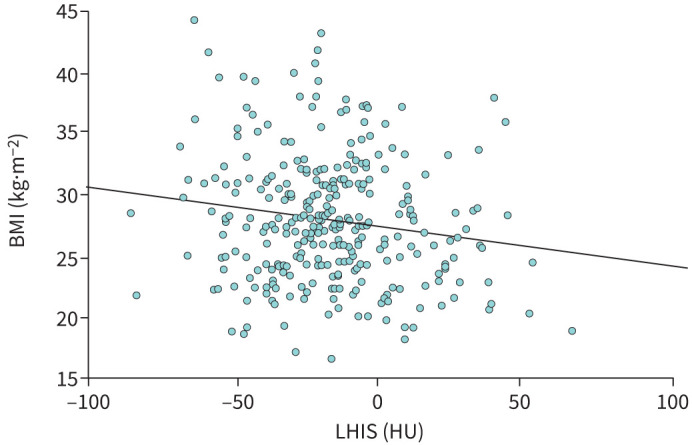
The prevalence of LHIS in all 5466 patients was 5.9%. 151 (72.6%) of 208 patients with COPD had LHIS. LHIS density in COPD patients was higher (-10.93 HU -21.1 HU; p<0.001), despite body mass index (BMI) (28.8 27.01 kg·m; p=0.002) being lower. LHIS density was lower in obese (BMI >30 kg·m) patients (20.4 13.6 HU; p=0.02). BMI was inversely correlated with LHIS density (BetaR -0.031; 95% CI: -0.054- -0.008; p=0.007). LHIS density was associated with COPD, but not with BMI on multivariate models. CAC and coronary stenosis severity (CADRADS and >50% stenosis) were not different (p=0.106, p=0.156 and p=0.350, respectively). HRPs were observed more frequently in COPD patients with severe Global Initiative for Chronic Obstructive Lung Disease (GOLD) stages ≥2 (32.3% 20.1%; p=0.044), but not when adding mild GOLD stages.
The prevalence of LHIS in COPD patients is high (72.6%), and the adipose tissue density is higher, indicating a higher brown fat component. In obese, patients LHIS density is lower and declines along with BMI. Coronary stenosis severity and calcium were not different; however HRPs were more frequent in severe COPD.
房间隔脂肪肥厚(LHIS)是心外膜脂肪组织的一个独特部分。然而,其与慢性阻塞性肺疾病(COPD)的关联鲜有文献记载。
回顾性招募因临床指征接受冠状动脉计算机断层扫描血管造影(CTA)的患者,筛查LHIS和COPD。通过CTA对LHIS密度和冠状动脉疾病特征进行量化:狭窄严重程度(冠状动脉疾病放射学报告系统(CADRADS))、冠状动脉钙化(CAC)和高危斑块(HRP)。将患有LHIS的COPD患者按年龄、性别、主要心血管危险因素(CVRFs)进行匹配,并与对照组进行比较。
在所有5466例患者中,LHIS的患病率为5.9%。208例COPD患者中有151例(72.6%)患有LHIS。尽管体重指数(BMI)较低(28.8对27.01kg·m²;p=0.002),但COPD患者的LHIS密度更高(-10.93HU对-21.1HU;p<0.001)。肥胖(BMI>30kg·m²)患者的LHIS密度较低(20.4对13.6HU;p=0.02)。BMI与LHIS密度呈负相关(βR -0.031;95%CI:-0.054至-0.008;p=0.007)。在多变量模型中,LHIS密度与COPD相关,但与BMI无关。CAC和冠状动脉狭窄严重程度(CADRADS和>50%狭窄)无差异(分别为p=0.106、p=0.156和p=0.350)。在慢性阻塞性肺疾病全球倡议(GOLD)≥2期的重度COPD患者中,HRP的观察频率更高(32.3%对20.1%;p=0.044),但加入轻度GOLD期时则不然。
COPD患者中LHIS的患病率较高(72.6%),且脂肪组织密度更高,表明棕色脂肪成分更多。在肥胖患者中,LHIS密度较低且随BMI下降。冠状动脉狭窄严重程度和钙化无差异;然而,重度COPD患者中HRP更常见。