Department of Medical Oncology, Bursa Yuksek Ihtisas Training and Research Hospital, University of Health Sciences, Bursa 16350, Turkey.
Department of Medical Oncology, School of Medicine, Bursa Uludag University, Bursa 16059, Turkey.
Curr Oncol. 2024 Sep 4;31(9):5195-5205. doi: 10.3390/curroncol31090384.
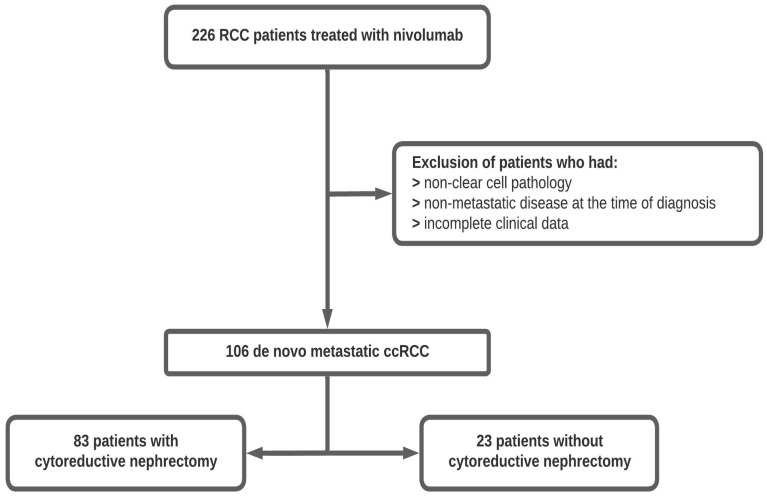
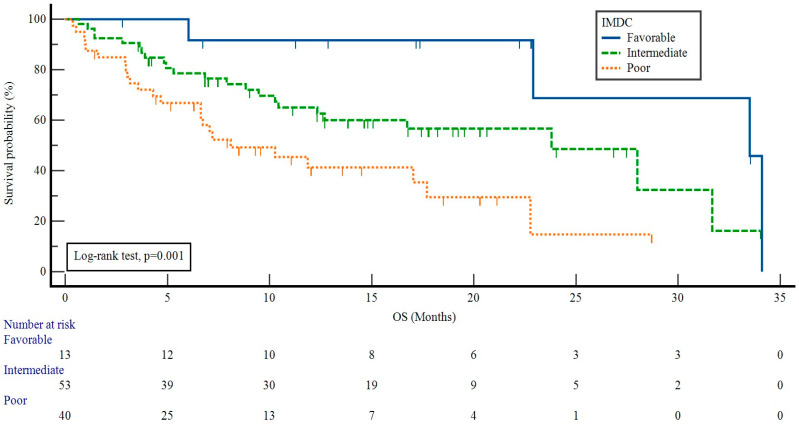
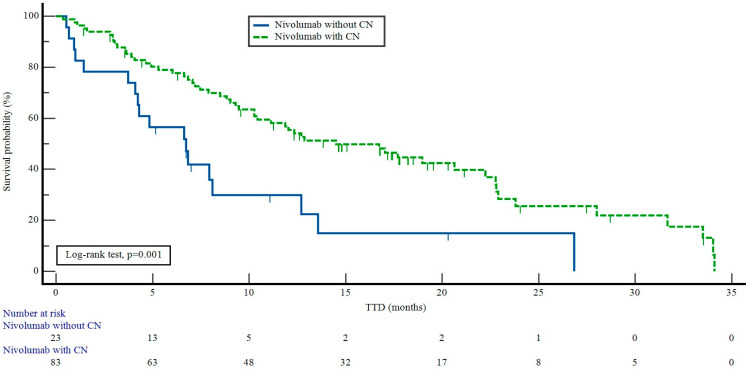
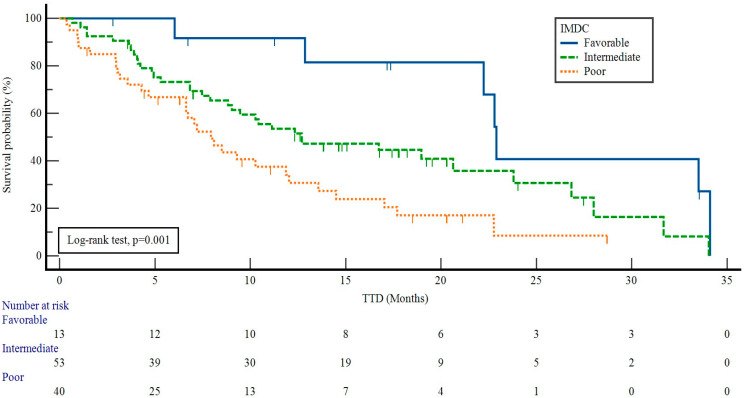
This study aimed to investigate the effect of cytoreductive nephrectomy (CN) on the survival outcomes of nivolumab used as a subsequent therapy after the failure of at least one anti-vascular endothelial growth factor (VEGF) agent in patients with metastatic clear-cell renal-cell carcinoma (ccRCC). We included 106 de novo metastatic ccRCC patients who received nivolumab after progression on at least one anti-VEGF agent. Multivariate Cox regression analysis was performed to investigate the factors affecting survival in patients receiving nivolumab. Of the 106 de novo metastatic ccRCC patients, 83 (78.3%) underwent CN. There were no statistical differences between the two groups in terms of age, gender, Eastern Cooperative Oncology Group (ECOG) score, tumor size, International Metastatic RCC Database Consortium (IMDC) risk group, number of previous treatment lines, first-line anti-VEGF therapy, or metastasis sites ( = 0.137, = 0.608, = 0.100, = 0.376, = 0.185, = 0.776, = 0.350, and = 0.608, respectively). The patients who received nivolumab with CN had a longer time to treatment discontinuation (TTD) [14.5 months, 95% confidence interval (CI): 8.6-20.3] than did those without CN 6.7 months (95% CI: 3.9-9.5) ( = 0.001). The median overall survival (OS) was 22.7 months (95% CI: 16.1-29.4). The patients with CN had a median OS of 22.9 months (95% CI: 16.3-29.4), while those without CN had a median OS of 8.1 months (95% CI: 5.6-10.5) ( = 0.104). In the multivariate analysis, CN [hazard ratio (HR): 0.521; 95% CI: 0.297-0.916; = 0.024] and the IMDC risk score ( = 0.011) were statistically significant factors affecting TTD; however, the IMDC risk score ( = 0.006) was the only significant factor for overall survival. Our study showed that the TTD of nivolumab was longer in metastatic ccRCC patients who underwent cytoreductive nephrectomy.
本研究旨在探讨细胞减积性肾切除术(CN)对至少一种抗血管内皮生长因子(VEGF)药物治疗失败后的转移性透明细胞肾细胞癌(ccRCC)患者接受nivolumab 作为后续治疗的生存结果的影响。我们纳入了 106 例新诊断为转移性 ccRCC 的患者,这些患者在至少一种抗 VEGF 药物治疗进展后接受了 nivolumab 治疗。多变量 Cox 回归分析用于研究接受 nivolumab 治疗的患者生存的影响因素。在 106 例新诊断为转移性 ccRCC 的患者中,83 例(78.3%)接受了 CN。两组在年龄、性别、东部合作肿瘤学组(ECOG)评分、肿瘤大小、国际转移性肾细胞癌数据库联盟(IMDC)风险组、治疗线数、一线抗 VEGF 治疗或转移部位方面无统计学差异(=0.137,=0.608,=0.100,=0.376,=0.185,=0.776,=0.350 和=0.608,分别)。接受 CN 联合 nivolumab 治疗的患者的治疗停药时间(TTD)[14.5 个月,95%置信区间(CI):8.6-20.3]长于未接受 CN 治疗的患者 6.7 个月(95%CI:3.9-9.5)(=0.001)。中位总生存期(OS)为 22.7 个月(95%CI:16.1-29.4)。接受 CN 的患者中位 OS 为 22.9 个月(95%CI:16.3-29.4),而未接受 CN 的患者中位 OS 为 8.1 个月(95%CI:5.6-10.5)(=0.104)。在多变量分析中,CN[风险比(HR):0.521;95%CI:0.297-0.916;=0.024]和 IMDC 风险评分(=0.011)是影响 TTD 的统计学显著因素;然而,IMDC 风险评分(=0.006)是影响总体生存的唯一显著因素。我们的研究表明,接受细胞减积性肾切除术的转移性 ccRCC 患者的 nivolumab 治疗停药时间更长。