Mattiolo Paola, Bevere Michele, Mafficini Andrea, Verschuur Anna Vera D, Calicchia Martina, Hackeng Wenzel M, Simbolo Michele, Paiella Salvatore, Dreijerink Koen M A, Landoni Luca, Pedron Serena, Cingarlini Sara, Salvia Roberto, Milella Michele, Lawlor Rita T, Valk Gerlof D, Vriens Menno R, Scarpa Aldo, Brosens Lodewijk A, Luchini Claudio
Department of Diagnostics and Public Health, Section of Pathology, University of Verona, Piazzale L.A. Scuro, 10, 37134, Verona, Italy.
ARC-NET Applied Research On Cancer Center, University of Verona, Verona, Italy.
Endocr Pathol. 2024 Dec;35(4):354-361. doi: 10.1007/s12022-024-09826-z. Epub 2024 Sep 27.
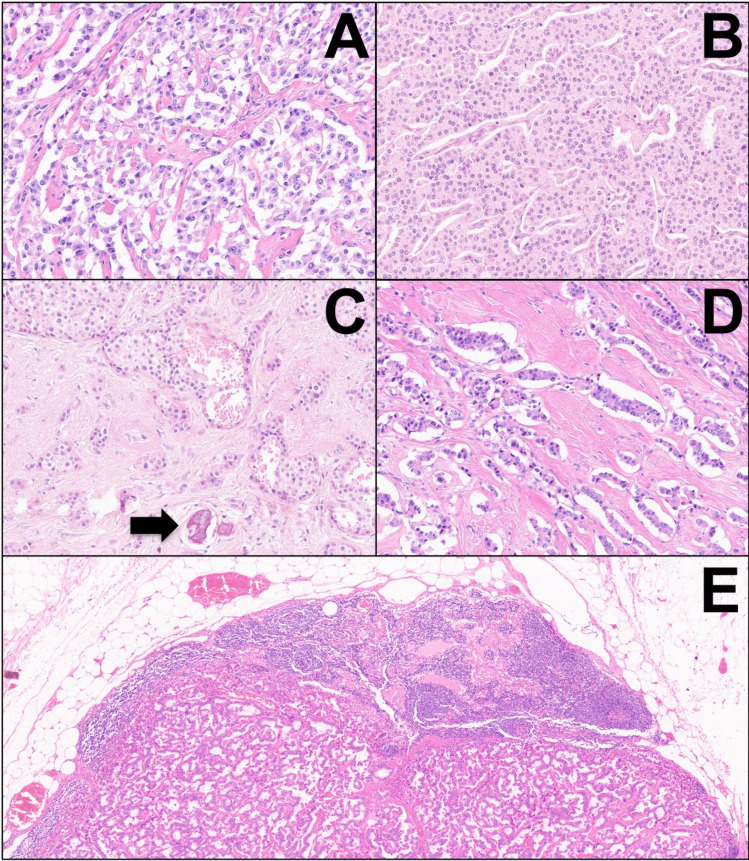
Glucagonomas are functioning pancreatic neuroendocrine tumors (PanNETs) responsible for glucagonoma syndrome. This study aims to shed light on the clinicopathological and molecular features of these neoplasms. Six patients with glucagonomas were identified. All neoplasms were investigated with immunohistochemistry for neuroendocrine markers (Synaptophysin, Chromogranin-A), ATRX, DAXX, ARX, and PDX1 transcription factors. Fluorescent in situ hybridization (FISH) for assessing alternative lengthening of telomeres (ALT), and next-generation sequencing (NGS) for molecular profiling were performed. All cases were large single masses (mean size of 8.2 cm), with necrolytic migratory erythema as the most common symptom (6/6 cases, 100%). All neoplasms were well-differentiated G1 tumors, except one case that was G2. The tumors consistently showed classic/conventional histomorphology, with solid-trabecular and nested architecture. Lymphatic and vascular invasion (6/6, 100%), perineural infiltration (4/6, 66.6%), and nodal metastasis (4/6, 66.6%) were frequently observed. Transcription factors expression showed strong ARX expression in all tumors, and PDX1 expression in 5/6 cases (83.3%), indicating co-occurring alpha- and beta-cell differentiation. NGS showed recurrent somatic MEN1 and ATRX/DAXX biallelic inactivation. Cases with ATRX or DAXX mutations also showed matched loss of ATRX or DAXX protein expression and ALT. One case harbored somatic MUTYH inactivation and showed a high tumor mutational burden (TMB, 41.0 mut/Mb). During follow-up, one patient died of the disease, and four patients developed distant metastasis. Pancreatic glucagonomas are distinct PanNETs with specific clinicopathological and molecular features, including histological aspects of biological aggressiveness, co-occurring alpha- and beta-cell differentiation, MEN1 and DAXX/ATRX mutations enrichment, and the possible presence of high-TMB as an actionable marker.
胰高血糖素瘤是引起胰高血糖素瘤综合征的功能性胰腺神经内分泌肿瘤(PanNETs)。本研究旨在阐明这些肿瘤的临床病理和分子特征。确定了6例胰高血糖素瘤患者。所有肿瘤均采用免疫组织化学方法检测神经内分泌标志物(突触素、嗜铬粒蛋白A)、ATRX、DAXX、ARX和PDX1转录因子。进行了用于评估端粒替代延长(ALT)的荧光原位杂交(FISH)和用于分子谱分析的下一代测序(NGS)。所有病例均为大的单发肿块(平均大小8.2 cm),坏死性游走性红斑是最常见症状(6/6例,100%)。除1例为G2级外,所有肿瘤均为高分化G1级肿瘤。肿瘤始终表现为经典/传统组织形态学,呈实性小梁状和巢状结构。经常观察到淋巴管和血管侵犯(6/6,100%)、神经周围浸润(4/6,66.6%)和淋巴结转移(4/6,66.6%)。转录因子表达显示所有肿瘤中ARX表达强烈,5/6例(83.3%)中有PDX1表达,表明同时存在α细胞和β细胞分化。NGS显示复发性体细胞MEN1和ATRX/DAXX双等位基因失活。ATRX或DAXX突变的病例也显示出ATRX或DAXX蛋白表达和ALT的匹配缺失。1例存在体细胞MUTYH失活,并显示出高肿瘤突变负荷(TMB,41.0突变/Mb)。在随访期间,1例患者死于该疾病,4例患者发生远处转移。胰腺胰高血糖素瘤是具有特定临床病理和分子特征的独特PanNETs,包括生物学侵袭性的组织学方面、同时存在的α细胞和β细胞分化、MEN1和DAXX/ATRX突变富集,以及可能存在高TMB作为可操作的标志物。