Vaduganathan Muthiah, Claggett Brian L, Desai Akshay S, Jhund Pardeep S, Lam Carolyn S P, Senni Michele, Shah Sanjiv J, Voors Adriaan A, Zannad Faiez, Pitt Bertram, Borentian Maria, Lay-Flurrie James, Viswanathan Prabhakar, Behmenburg Friederike U, McMurray John J V, Solomon Scott D
Brigham and Women's Hospital, Harvard Medical School, Boston, Massachusetts.
University of Glasgow, Glasgow, Scotland, United Kingdom.
JAMA Cardiol. 2025 Feb 1;10(2):176-181. doi: 10.1001/jamacardio.2024.3782.
People living with heart failure (HF) with mildly reduced or preserved ejection fraction have substantially curtailed life expectancy free from clinical events compared with their peers of comparable age. The nonsteroidal mineralocorticoid receptor antagonist, finerenone, was recently shown to reduce risks of cardiovascular events in this population over a median follow-up of 2.6 years; as patients with HF typically continue treatment beyond this time frame, estimating the potential long-term benefits of finerenone could inform shared clinical decision-making.
To estimate the projected long-term treatment effects of finerenone in patients with HF with mildly reduced or preserved ejection fraction if treated over a patient's lifetime.
DESIGN, SETTING, AND PARTICIPANTS: Prespecified analyses were conducted of the FINEARTS-HF trial, a phase 3 randomized clinical trial conducted across 653 sites in 37 countries. Adults 40 years and older with symptomatic HF and left ventricular ejection fraction of 40% or greater were randomized from September 2020 to January 2023. Median (IQR) follow-up was 2.6 (1.9-3.0) years.
Finerenone (titrated to either 20 mg or 40 mg) or placebo.
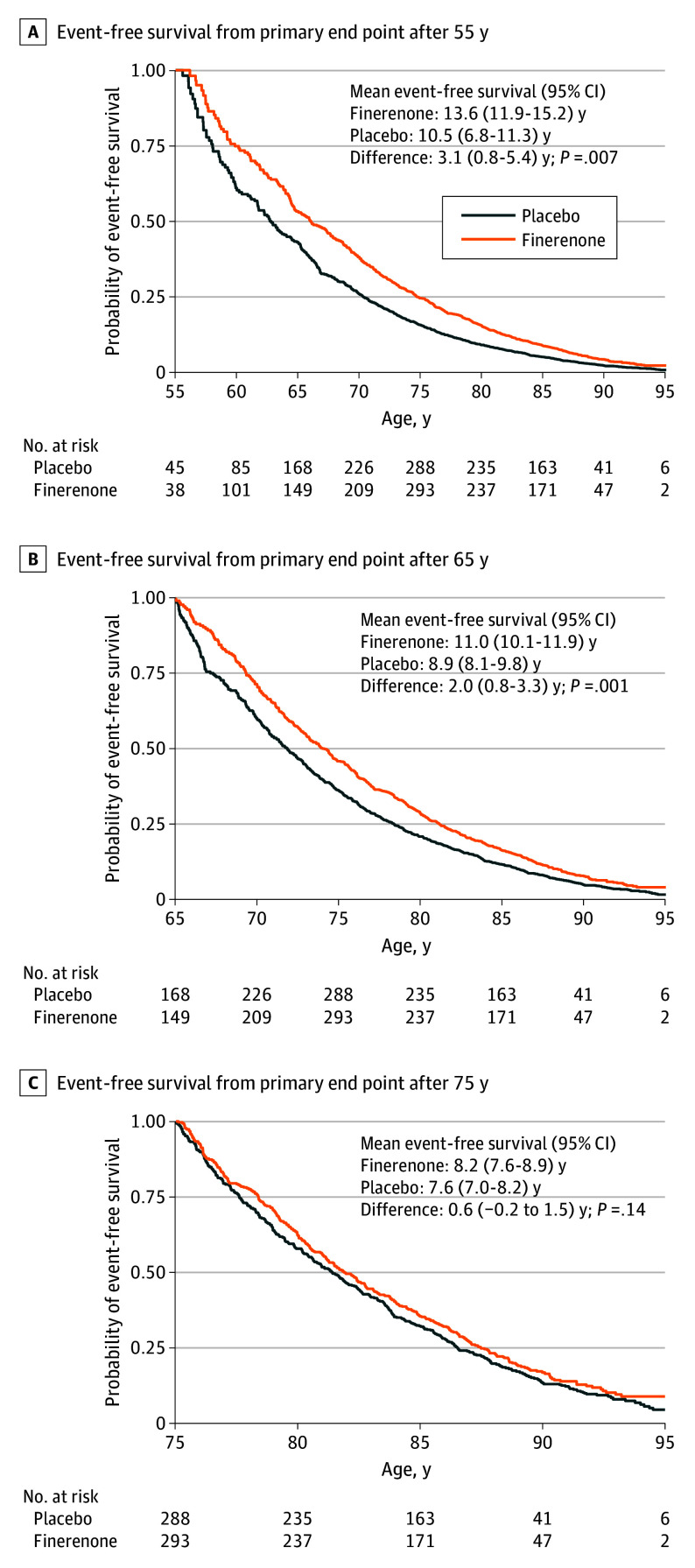
The primary composite outcome was time to cardiovascular death or worsening HF event. The long-term gains in survival free from a primary end point with finerenone were iteratively estimated with age-based Kaplan-Meier curves using age at randomization rather than time from randomization. Differences in areas under the survival curves between the finerenone and placebo arms represented event-free survival gains.
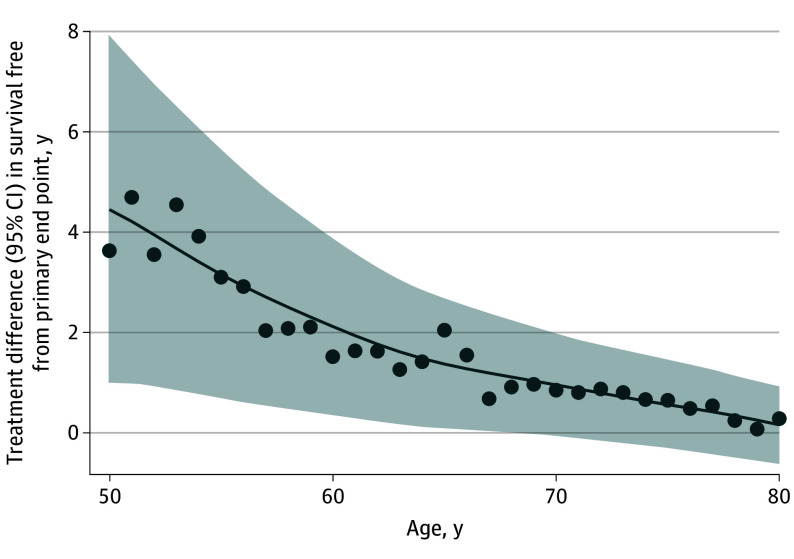
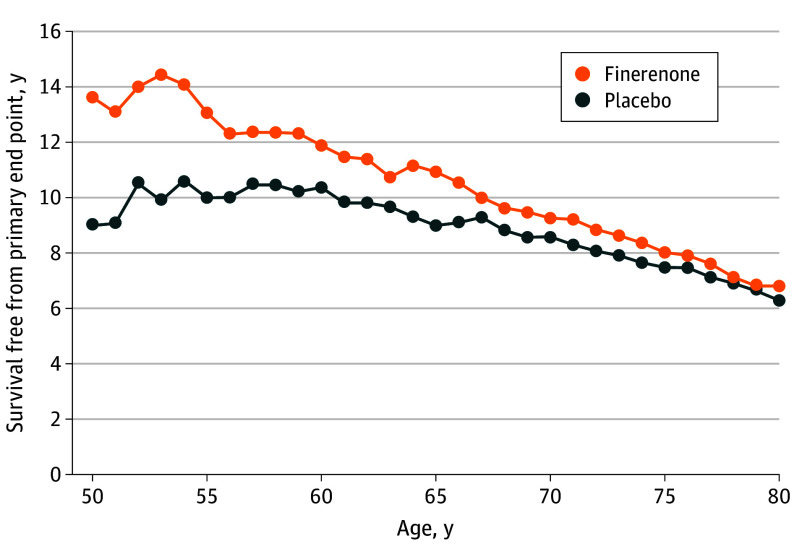
Among 6001 participants (median [IQR] age, 73 [66-79] years; 3269 male [54.5%]), mean survival free from the primary end point for a 55-year-old participant was 13.6 years (95% CI, 11.9-15.2 years) with finerenone and 10.5 years (95% CI, 6.8-11.3 years) with placebo, representing a gain in event-free survival of 3.1 years (95% CI, 0.8-5.4 years; P = .007). Mean event-free survival for a 65-year-old participant was 11.0 years (95% CI, 10.1-11.9 years) with finerenone and 8.9 years (95% CI, 8.1-9.8 years) with placebo, representing a gain of 2.0 years (95% CI, 0.8-3.3 years; P = .001). Projected mean event-free survival was numerically greater with finerenone than with placebo for every starting age between 50 to 80 years. Lifetime gains in event-free survival were observed even among individuals already treated with a sodium-glucose cotransporter 2 inhibitor (65-year-old participant: 3.1 years; 95% CI, 0.1-6.0 years; P = .04).
In this prespecified secondary analysis of the FINEARTS-HF randomized clinical trial, long-term treatment with finerenone was estimated to extend event-free survival by up to 3 years among people with HF with mildly reduced or preserved ejection fraction.
ClinicalTrials.gov Identifier: NCT04435626.
与年龄相仿的同龄人相比,射血分数轻度降低或保留的心力衰竭(HF)患者无临床事件的预期寿命大幅缩短。非甾体类盐皮质激素受体拮抗剂非奈利酮最近显示,在中位随访2.6年期间可降低该人群发生心血管事件的风险;由于HF患者通常在此时间框架后仍继续接受治疗,评估非奈利酮的潜在长期益处可为临床共同决策提供依据。
评估非奈利酮在射血分数轻度降低或保留的HF患者中进行终身治疗的预计长期治疗效果。
设计、设置和参与者:对FINEARTS-HF试验进行了预先指定的分析,这是一项在37个国家的653个地点进行的3期随机临床试验。2020年9月至2023年1月,将40岁及以上有症状HF且左心室射血分数为40%或更高的成年人随机分组。中位(IQR)随访时间为2.6(1.9-3.0)年。
非奈利酮(滴定至20mg或40mg)或安慰剂。
主要复合结局为心血管死亡或HF事件恶化的时间。使用随机分组时的年龄而非随机分组后的时间,通过基于年龄的Kaplan-Meier曲线迭代估计非奈利酮在无主要终点生存方面的长期获益。非奈利酮组和安慰剂组生存曲线下面积的差异代表无事件生存获益。
在6001名参与者中(中位[IQR]年龄,73[66-79]岁;3269名男性[54.5%]),对于一名55岁的参与者,接受非奈利酮治疗无主要终点的平均生存期为13.6年(95%CI,11.9-15.2年),接受安慰剂治疗为10.5年(95%CI,6.8-11.3年),无事件生存获益为3.1年(95%CI,0.8-5.4年;P = 0.007)。对于一名65岁的参与者,接受非奈利酮治疗的平均无事件生存期为11.0年(95%CI,10.1-11.9年),接受安慰剂治疗为8.9年(95%CI,8.1-9.8年),获益为2.0年(95%CI,0.8-3.3年;P = 0.001)。在50至80岁之间的每个起始年龄,非奈利酮预计的平均无事件生存期在数值上均高于安慰剂。即使在已经接受钠-葡萄糖协同转运蛋白2抑制剂治疗的个体中也观察到了无事件生存的终身获益(65岁参与者:3.1年;95%CI,0.1-6.0年;P = 0.04)。
在这项对FINEARTS-HF随机临床试验的预先指定的二次分析中,估计非奈利酮长期治疗可使射血分数轻度降低或保留的HF患者的无事件生存期延长多达3年。
ClinicalTrials.gov标识符:NCT04435626。