Plessi Carlotta, Tambucci Roberto, Reding Raymond, Stephenne Xavier, Scheers Isabelle, Jannone Giulia, de Magnée Catherine
Pediatric Surgery and Transplantation Unit, Department of Surgery, Cliniques Universitaires Saint-Luc, ERN TransplantChild, ERN Rare Liver, Université Catholique de Louvain, 1200 Brussels, Belgium.
Pediatric Gastroenterology and Hepatology Unit, Department of Pediatrics, Cliniques Universitaires Saint-Luc, ERN TransplantChild, ERN Rare Liver, Université Catholique de Louvain, 1200 Brussels, Belgium.
Children (Basel). 2024 Sep 3;11(9):1079. doi: 10.3390/children11091079.
BACKGROUND/OBJECTIVES: Liver retransplantation (reLT) is the only option for pediatric patients experiencing graft loss. Despite recent advancements in surgical techniques and perioperative management, it remains a high-risk procedure. Our aim is to describe our experience in pediatric reLT, focusing on the technical aspects and surgical challenges.
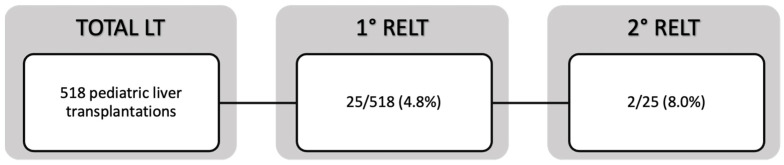
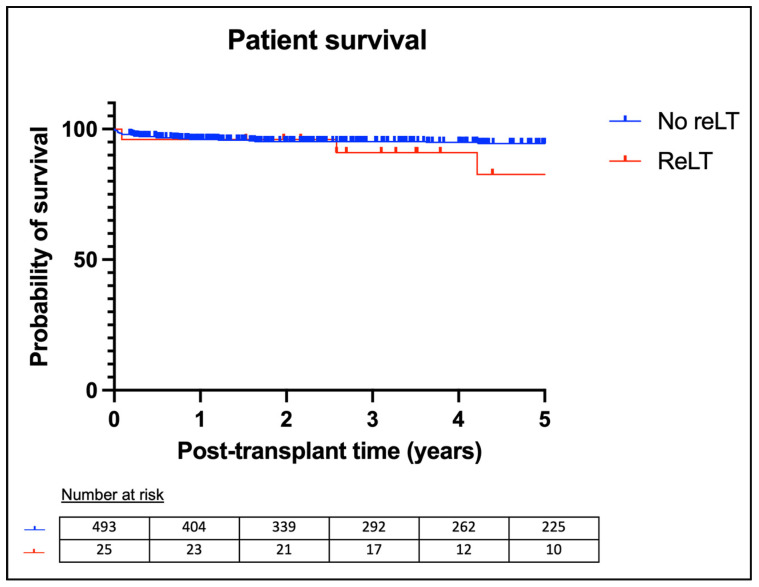
We systematically analyzed surgical reports from pediatric reLT performed at our center between 2006 and 2023 to identify recurrent intraoperative findings and specific surgical techniques. We focused on challenges encountered during different phases of reLT, including hepatectomy, vascular, and biliary reconstruction. Additionally, we compared patient and graft survival rates among different groups.
During the study period, 23 children underwent 25 reLT procedures at our center. Major surgical challenges included complex hepatectomy and vascular reconstructions, necessitating tailored approaches. Our analysis shows that patient and graft survival were significantly lower for reLT compared to primary transplantation ( = 0.002). Early reLT had a significantly lower graft survival compared to late reLT ( = 0.002), although patient survival was comparable ( = 0.278). Patient and graft survival rates were comparable between the first and second reLT ( = 0.300, = 0.597). Patient survival tended to be higher after living-donor liver transplantation (LDLT) compared to deceased-donor liver transplantation (DDLT), although the difference was not statistically significant ( = 0.511).
Pediatric reLT involves significant technical challenges and lower survival rates. Advances in perioperative management are crucial for improving outcomes. Further research is needed to optimize surgical strategies and evaluate the long-term benefits of LDLT in pediatric reLT.
背景/目的:肝再次移植(reLT)是小儿移植肝失功患者的唯一选择。尽管手术技术和围手术期管理最近有所进步,但它仍然是一项高风险手术。我们的目的是描述我们在小儿肝再次移植方面的经验,重点关注技术方面和手术挑战。
我们系统分析了2006年至2023年在本中心进行的小儿肝再次移植手术报告,以确定术中反复出现的发现和特定的手术技术。我们重点关注肝再次移植不同阶段遇到的挑战,包括肝切除术、血管和胆道重建。此外,我们比较了不同组的患者和移植肝生存率。
在研究期间,23名儿童在本中心接受了25次肝再次移植手术。主要的手术挑战包括复杂的肝切除术和血管重建,需要采用定制的方法。我们的分析表明,与初次移植相比,肝再次移植的患者和移植肝生存率显著降低(P = 0.002)。早期肝再次移植的移植肝生存率明显低于晚期肝再次移植(P = 0.002),尽管患者生存率相当(P = 0.278)。首次和第二次肝再次移植的患者和移植肝生存率相当(P = 0.300,P = 0.597)。与尸体供肝肝移植(DDLT)相比,活体供肝肝移植(LDLT)后的患者生存率往往更高,尽管差异无统计学意义(P = 0.511)。
小儿肝再次移植涉及重大技术挑战且生存率较低。围手术期管理的进步对于改善结局至关重要。需要进一步研究以优化手术策略并评估活体供肝肝移植在小儿肝再次移植中的长期益处。