Caliskan Etem, Misfeld Martin, Sandner Sigrid, Böning Andreas, Aramendi Jose, Salzberg Sacha P, Choi Yeong-Hoon, Perrault Louis P, Tekin Ilker, Cuerpo Gregorio P, Lopez-Menendez Jose, Weltert Luca P, Böhm Johannes, Krane Markus, González-Santos José M, Tellez Juan-Carlos, Holubec Tomas, Ferrari Enrico, Doros Gheorghe, Emmert Maximilian Y
Department of Cardiothoracic and Vascular Surgery, Deutsches Herzzentrum der Charité (DHZC), Berlin, Germany.
Charité-Universitätsmedizin Berlin, Corporate Member of Freie Universität Berlin and Humboldt-Universität zu Berlin, Berlin, Germany.
Front Cardiovasc Med. 2024 Sep 12;11:1366460. doi: 10.3389/fcvm.2024.1366460. eCollection 2024.
Although cardiovascular surgery societies in Europe and the USA constantly strive for the exchange of knowledge and best practices in coronary artery bypass grafting (CABG), the available evidence on whether such efforts result in similar patient outcomes is limited. Therefore, in the present analysis, we sought to compare patient profiles and overall survival outcomes for up to 3 years between large European and US patient cohorts who underwent isolated CABG.
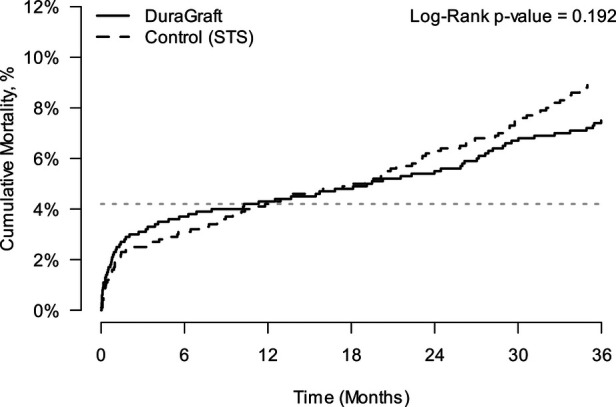
Patients from the European DuraGraft Registry ( = 2,522) who underwent isolated CABG at 45 sites in eight different European countries between 2016 and 2019 were compared to randomly selected patients from the US STS database who were operated during the same period ( = 294,725). Free conduits (venous and arterial grafts) from the DuraGraft Registry patients were intraoperatively stored in DuraGraft, an endothelial damage inhibitor, before anastomosis, whereas grafts from the STS Registry patients in standard-of-care solutions (e.g., saline). Propensity score matching (PSM) models were used to account for differences in patient baseline and surgical characteristics, using a primary PSM with 35 variables (2,400 patients matched) and a secondary PSM with 25 variables (2,522 patients matched, sensitivity analysis). The overall survival for up to 3 years after CABG was assessed as the primary endpoint.
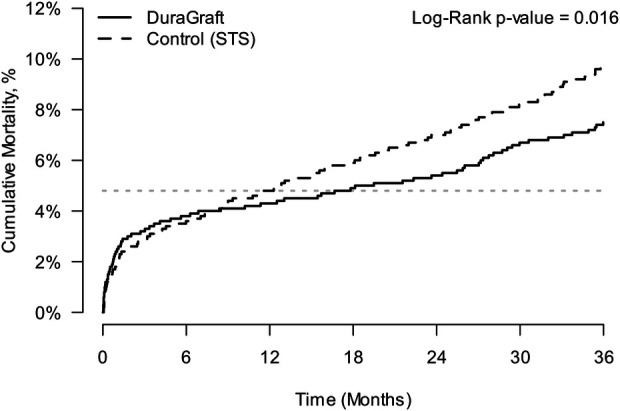
The comparison of patient profiles showed significant differences between the European and US cohorts. The European patients had more left main disease, underwent more off-pump CABG, and received more arterial grafts together with more complete arterial grafting procedures. In contrast, the US patients received more distal anastomoses with more saphenous vein grafts (SVGs) that were mainly harvested endoscopically. Such differences, however, were well balanced after PSM for the mortality comparison. Mortality comparison at 30 days, 12 months, and 24 months between the European and US patients was 2.38% vs. 1.96%, 4.32% vs. 4.79%, and 5.38% vs. 6.96%, respectively. At 36 months, the mortality was significantly lower in the European patients than that of their US counterparts (7.37% vs. 9.65%; -value = 0.016). The estimated hazard ratio (HR) was 1.29 (95% CI 1.05-1.59).
This large-scale transatlantic comparative analysis shows that there are some significant differences in patient profiles between large cohorts of European and US patients. These differences were adjusted by using PSM for the mortality analysis. No significant difference in mortality was detected between groups through 2 years, but survival was significantly better in the European DuraGraft Registry patients at 3 years post-CABG.
尽管欧洲和美国的心血管外科学会一直在努力促进冠状动脉旁路移植术(CABG)知识和最佳实践的交流,但关于这些努力是否能带来相似的患者预后的现有证据有限。因此,在本分析中,我们试图比较接受单纯CABG的欧洲和美国大型患者队列之间的患者特征和长达3年的总体生存结局。
将2016年至2019年期间在八个不同欧洲国家的45个地点接受单纯CABG的欧洲DuraGraft注册研究中的患者(n = 2,522)与同期在美国STS数据库中随机选择的接受手术的患者(n = 294,725)进行比较。DuraGraft注册研究患者的游离血管(静脉和动脉移植物)在吻合前术中储存在内皮损伤抑制剂DuraGraft中,而STS注册研究患者的移植物则储存在标准护理溶液(如生理盐水)中。倾向评分匹配(PSM)模型用于解释患者基线和手术特征的差异,使用包含35个变量的主要PSM(匹配2,400例患者)和包含25个变量的次要PSM(匹配2,522例患者,敏感性分析)。将CABG后长达3年的总体生存作为主要终点进行评估。
患者特征比较显示欧洲和美国队列之间存在显著差异。欧洲患者左主干病变更多,接受非体外循环CABG更多,接受动脉移植物更多且动脉移植物完全性手术更多。相比之下,美国患者进行更多的远端吻合,使用更多的大隐静脉移植物(SVG),且主要通过内镜获取。然而,在PSM后进行死亡率比较时,这些差异得到了很好的平衡。欧洲和美国患者在30天、12个月和24个月时的死亡率比较分别为2.38%对1.96%、4.32%对4.79%和5.38%对6.96%。在36个月时,欧洲患者的死亡率显著低于美国患者(7.37%对9.65%;P值 = 0.016)。估计风险比(HR)为1.29(95%CI 1.05 - 1.59)。
这项大规模的跨大西洋比较分析表明,欧洲和美国大型患者队列之间的患者特征存在一些显著差异。通过使用PSM对死亡率分析进行了调整。在2年内各组之间未检测到死亡率的显著差异,但CABG术后3年欧洲DuraGraft注册研究患者的生存率显著更好。