Flausino Lucas E, Ferreira Isabella N, Tuan Wen-Jan, Estevez-Diz Maria Del Pilar, Chammas Roger
Center for Translational Research in Oncology, Instituto do Câncer do Estado de São Paulo, Faculdade de Medicina da Universidade de São Paulo, Comprehensive Center for Precision Oncology, Universidade de São Paulo, São Paulo, SP, Brazil.
Department of Family and Community Medicine, and Public Health Sciences, Penn State College of Medicine, Hershey, PA, United States.
Front Oncol. 2024 Sep 13;14:1433497. doi: 10.3389/fonc.2024.1433497. eCollection 2024.
We conducted an extensive, sex-oriented real-world data analysis to explore the impact and safety of non-steroidal anti-inflammatory drugs (NSAIDs) and selective COX-2 inhibitors (coxibs) on cancer treatment outcomes. This is particularly relevant given the role of the COX-2/PGE2 pathway in tumor cell resistance to chemotherapy and radiotherapy.
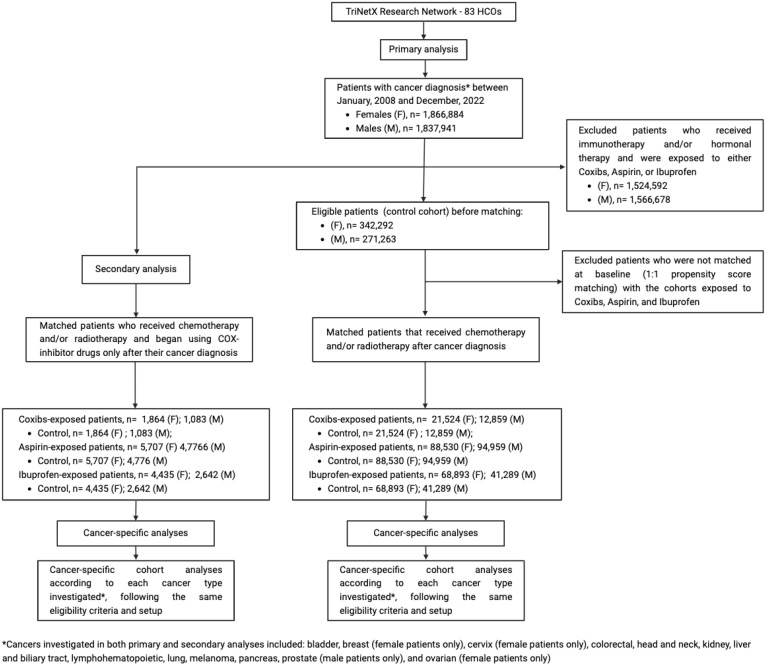
The study applied a retrospective cohort design utilizing the TriNetX research database consisting of patients receiving cancer treatment in 2008-2022. The treated cohorts included patients who were prescribed with coxibs, aspirin or ibuprofen, while individuals in the control cohort did not receive these medicines during their cancer treatment. A 1:1 propensity score matching technique was used to balance the baseline characteristics in the treated and control cohorts. Then, Cox proportional hazards regression and logistic regression were applied to assess the mortality and morbidity risks among patient cohorts in a 5-year follow-up period.
Use of coxibs (HR, 0.825; 95% CI 0.792-0.859 in females and HR, 0.884; 95% CI 0.848-0.921 in males) and ibuprofen (HR, 0.924; 95% CI 0.903-0.945 in females and HR, 0.940; 95% CI 0.917-0.963 in males) were associated with improved survival. Female cancer patients receiving aspirin presented increased mortality (HR, 1.078; 95% CI 1.060-1.097), while male cancer patients also had improved survival when receiving aspirin (HR, 0.966; 95% CI 0.951-0.980). Cancer subtype specific analysis suggests coxibs and ibuprofen correlated with survival, though ibuprofen and aspirin increased emergency department visits' risk. Secondary analyses, despite limited by small cohort sizes, suggest that COX inhibition post-cancer diagnosis may benefit patients with specific cancer subtypes.
Selective COX-2 inhibition significantly reduced mortality and emergency department visit rates. Further clinical trials are needed to determine the optimal conditions for indication of coxibs as anti-inflammatory adjuvants in cancer treatment.
我们进行了一项广泛的、以性别为导向的真实世界数据分析,以探讨非甾体抗炎药(NSAIDs)和选择性COX-2抑制剂(coxibs)对癌症治疗结果的影响和安全性。鉴于COX-2/PGE2途径在肿瘤细胞对化疗和放疗的耐药性中的作用,这一点尤为重要。
该研究采用回顾性队列设计,利用TriNetX研究数据库,该数据库包含2008年至2022年接受癌症治疗的患者。治疗队列包括开具了coxibs、阿司匹林或布洛芬的患者,而对照队列中的个体在癌症治疗期间未接受这些药物。采用1:1倾向评分匹配技术来平衡治疗队列和对照队列的基线特征。然后,应用Cox比例风险回归和逻辑回归来评估患者队列在5年随访期内的死亡率和发病率风险。
使用coxibs(女性的HR为0.825;95%CI为0.792-0.859,男性的HR为0.884;95%CI为0.848-0.921)和布洛芬(女性的HR为0.924;95%CI为0.903-0.945,男性的HR为0.940;95%CI为0.917-0.963)与生存率提高相关。接受阿司匹林治疗的女性癌症患者死亡率增加(HR为1.078;95%CI为1.060-1.097),而接受阿司匹林治疗的男性癌症患者生存率也有所提高(HR为0.966;95%CI为0.951-0.980)。癌症亚型特异性分析表明,coxibs和布洛芬与生存率相关,尽管布洛芬和阿司匹林增加了急诊就诊风险。二次分析尽管受限于队列规模较小,但表明癌症诊断后抑制COX可能使特定癌症亚型的患者受益。
选择性COX-2抑制显著降低了死亡率和急诊就诊率。需要进一步的临床试验来确定将coxibs作为癌症治疗中抗炎佐剂的最佳适应症条件。