He Fang, Chen Mo, Yao Qi-Jun, Liu Zhi-Min, Zhao Yandong, Pei Fengyun, Zheng Jian, Gao Yuan-Hong, Huang Jun
Department of Radiation Oncology, Sun Yat-sen University Cancer Centre, State Key Laboratory of Oncology in South China, Collaborative Innovation Centre for Cancer Medicine, Guangzhou, Guangdong, China; Department of Radiation Oncology, Guangdong Provincial Key Laboratory of Colorectal and Pelvic Floor Diseases, The Sixth Affiliated Hospital, Sun Yat-sen University, Guangzhou, Guangdong, China; Biomedical Innovation Centre, The Sixth Affiliated Hospital, Sun Yat-sen University, Guangzhou, Guangdong, China.
Department of Genitourinary oncology, The First People's Hospital of Foshan, Foshan, Guangdong, China.
Transl Oncol. 2024 Dec;50:102133. doi: 10.1016/j.tranon.2024.102133. Epub 2024 Sep 30.
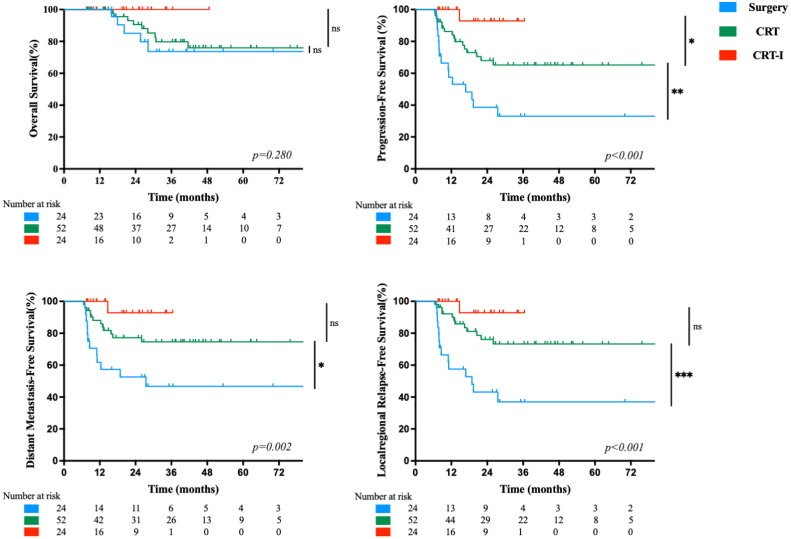
The current standard of care for anal squamous cell carcinoma (ASCC) is definitive concurrent chemoradiotherapy (CRT). However, about a third of patients may experience treatment failure. Recently, immunotherapy has emerged as a novel strategy for metastatic ASCC patients. We evaluated the efficacy and safety of surgery, CRT alone, and CRT with immunotherapy (CRT-I) in 100 nonmetastatic ASCC patients, treated from April 2012 through May 2023, by determining survival outcomes and acute adverse events. The median (range) follow-up was 30.7 (7.6 to 134.9) months. The study cohort 3-year overall survival (OS), progression-free survival (PFS), distant metastasis-free survival (DMFS), and locoregional recurrence-free survival (LRFS) rates were 80.7 %, 62.2 %, 71.1 %, and 67.6 %, respectively. The Surgery group had significantly lower rates than the CRT and CRT-I groups for 3-year PFS (33.1% vs. 65.2% vs. 92.9 %, P < 0.001), DMFS (46.7% vs. 74.6% vs. 92.9 %, P = 0.002) and LRFS (37.0% vs. 73.3% vs. 92.9 %, P < 0.001), respectively. All patients receiving CRT-I were alive at last follow-up. Of 100 patients, 26 (26.0 %) experienced severe (≥ grade 3) acute toxicity. Of 24 patients receiving CRT-I, 8 (33.3 %) had severe acute toxicity. Using immunohistochemistry, peritumoural stromal infiltration by CD8+ T cells was significantly higher after CRT-I compared to before CRT-I and to after CRT alone. The addition of immunotherapy to CRT may be an effective first-line treatment option with favourable survival outcomes and acceptable toxicity for patients with ASCC. A prospective, randomized trial assessing the efficacy of CRT combined with a PD-1 inhibitor in patients with locally advanced ASCC is in progress.
肛管鳞状细胞癌(ASCC)目前的标准治疗方案是确定性同步放化疗(CRT)。然而,约三分之一的患者可能会出现治疗失败。最近,免疫疗法已成为转移性ASCC患者的一种新策略。我们通过确定生存结局和急性不良事件,评估了2012年4月至2023年5月期间接受治疗的100例非转移性ASCC患者接受手术、单纯CRT以及CRT联合免疫疗法(CRT-I)的疗效和安全性。中位(范围)随访时间为30.7(7.6至134.9)个月。研究队列的3年总生存率(OS)、无进展生存率(PFS)、无远处转移生存率(DMFS)和无局部区域复发生存率(LRFS)分别为80.7%、62.2%、71.1%和67.6%。手术组的3年PFS(33.1%对65.2%对92.9%,P<0.001)、DMFS(46.7%对74.6%对92.9%,P = 0.002)和LRFS(37.0%对73.3%对92.9%,P<0.001)率均显著低于CRT组和CRT-I组。所有接受CRT-I的患者在最后一次随访时均存活。100例患者中,26例(26.0%)出现严重(≥3级)急性毒性反应。在接受CRT-I的24例患者中,8例(33.3%)出现严重急性毒性反应。使用免疫组织化学方法检测发现,与CRT-I治疗前及单纯CRT治疗后相比,CRT-I治疗后肿瘤周围CD8+T细胞的基质浸润显著增加。对于ASCC患者,在CRT基础上加用免疫疗法可能是一种有效的一线治疗选择,具有良好的生存结局和可接受的毒性。一项评估CRT联合PD-1抑制剂治疗局部晚期ASCC患者疗效的前瞻性随机试验正在进行中。