Centre for Biomedical Engineering, Indian Institute of Technology Delhi, New Delhi, India.
Medical Oncology, Dr. B.R.A. Institute Rotary Cancer Hospital, All India Institute of Medical Sciences, New Delhi, India.
Sci Rep. 2024 Oct 1;14(1):22811. doi: 10.1038/s41598-024-71173-0.
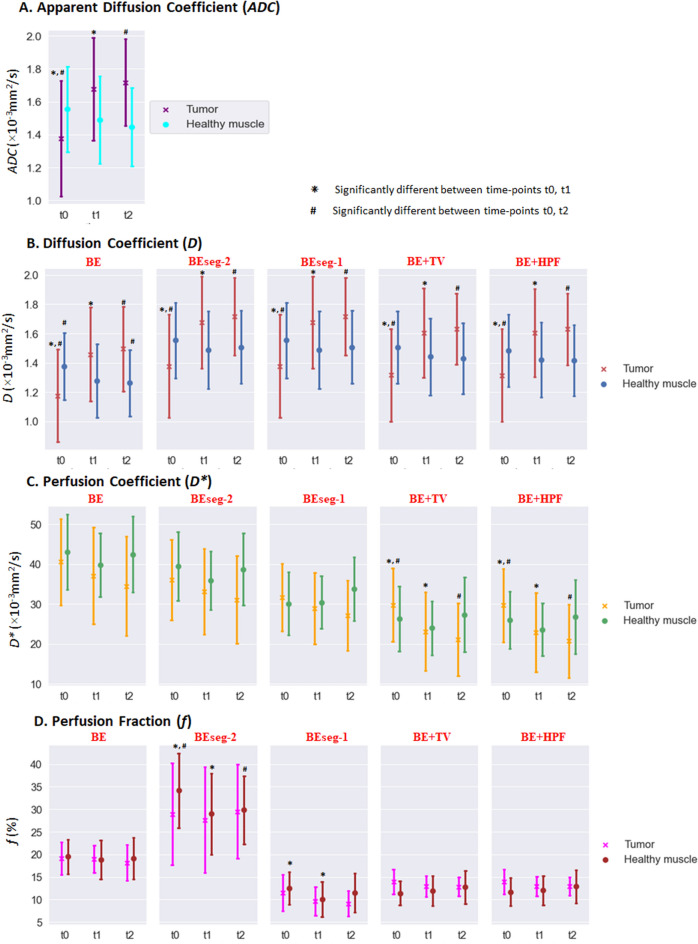
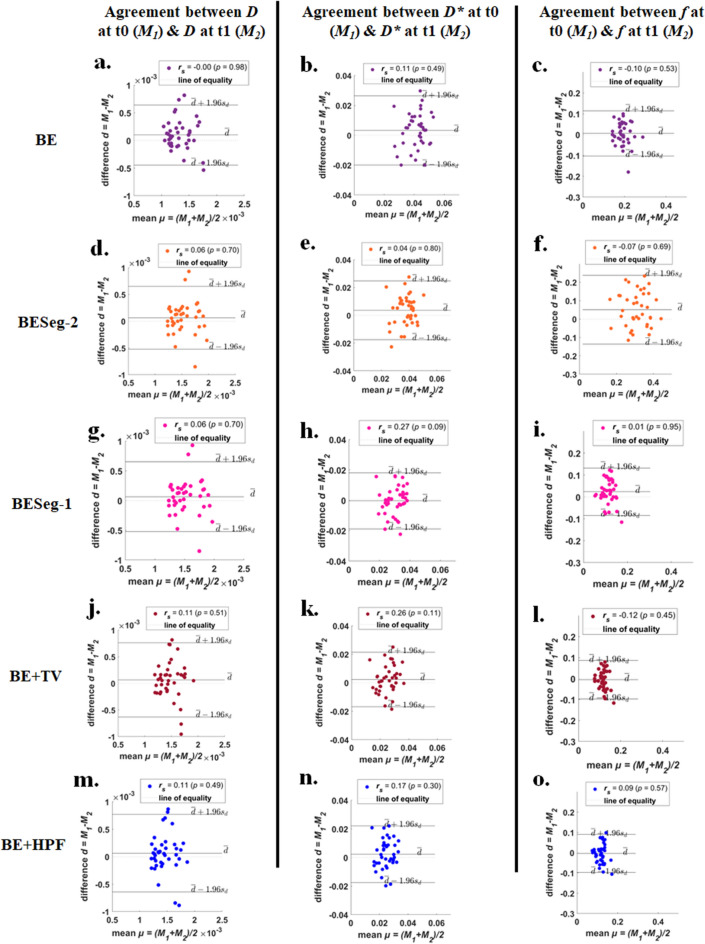
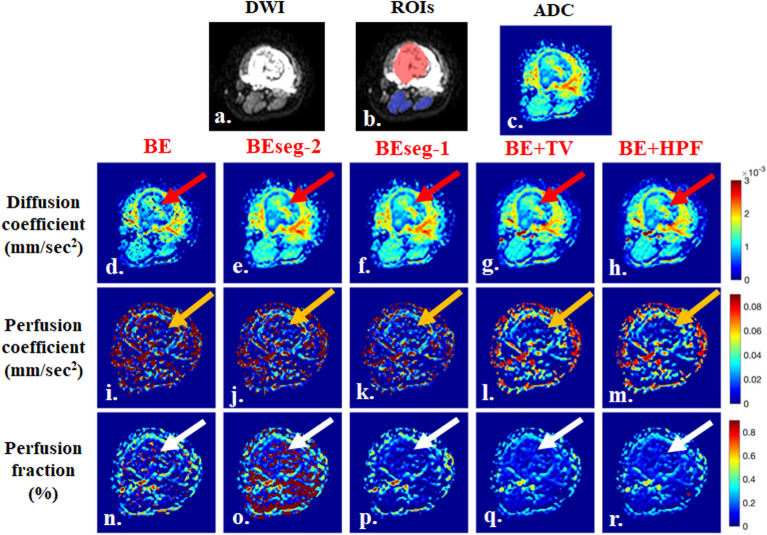
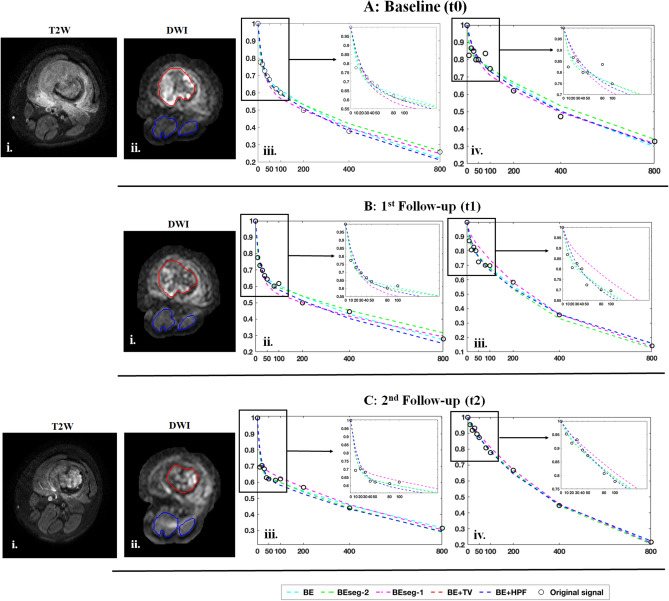
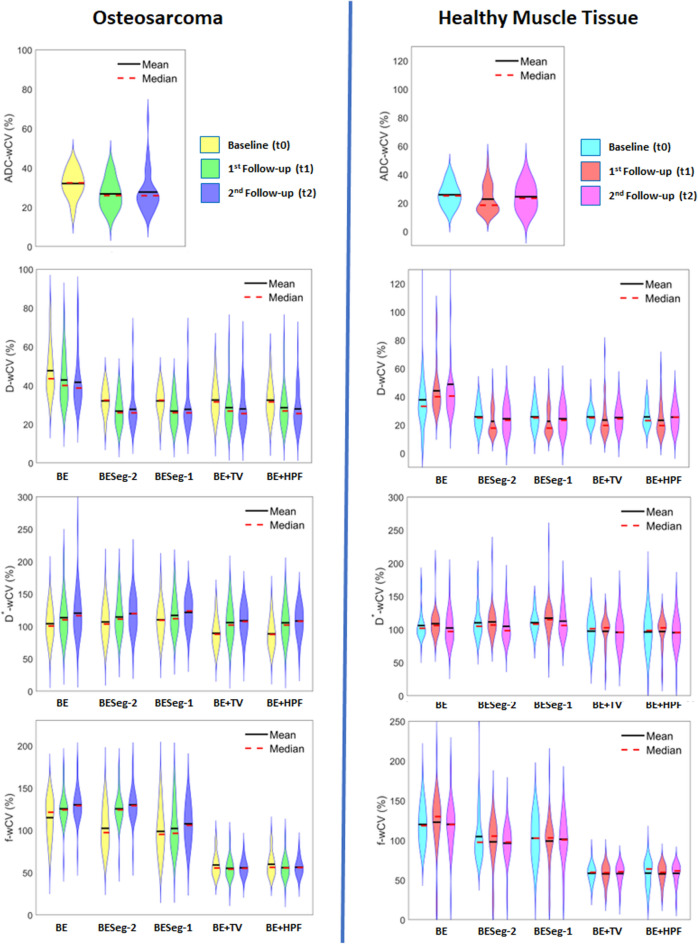
Objective was to assess the precision and reproducibility of spatial penalty-based intravoxel incoherent motion (IVIM) methods in comparison to the conventional bi-exponential (BE) model-based IVIM methods. IVIM-MRI (11 b-values; 0-800 s/mm) of forty patients (N = 40; Age = 17.7 ± 5.9 years; Male:Female = 30:10) with biopsy-proven osteosarcoma were acquired on a 1.5 Tesla scanner at 3 time-points: (i) baseline, (ii) after 1-cycle and (iii) after 3-cycles of neoadjuvant chemotherapy. Diffusion coefficient (D), Perfusion coefficient (D*) and Perfusion fraction (f) were estimated at three time-points in whole tumor and healthy muscle tissue using five methodologies (1) BE with three-parameter-fitting (BE), (2) Segmented-BE with two-parameter-fitting (BESeg-2), (3) Segmented-BE with one-parameter-fitting (BESeg-1), (4) BE with adaptive Total-Variation-penalty (BE + TV) and (5) BE with adaptive Huber-penalty (BE + HPF). Within-subject coefficient-of-variation (wCV) and between-subject coefficient-of-variation (bCV) of IVIM parameters were measured in healthy and tumor tissue. For precision and reproducibility, intra-scan comparison of wCV and bCV among five IVIM methods were performed using Friedman test followed by Wilcoxon-signed-ranks (WSR) post-hoc test. Experimental results demonstrated that BE + TV and BE + HPF showed significantly (p < 10) lower wCV and bCV for D (wCV: 24-32%; bCV: 22-31%) than BE method (wCV: 38-49%; bCV: 36-46%) across three time-points in healthy muscle and tumor. BE + TV and BE + HPF also demonstrated significantly (p < 10) lower wCV and bCV for estimating D* (wCV: 89-108%; bCV: 83-102%) and f (wCV: 55-60%; bCV: 56-60%) than BE, BESeg-2 and BESeg-1 methods (D*-wCV: 102-122%; D*-bCV: 98-114% and f-wCV: 96-130%; f-bCV: 94-125%) in both tumor and healthy tissue across three time-points. Spatial penalty based IVIM analysis methods BE + TV and BE + HPF demonstrated lower variability and improved precision and reproducibility in the current clinical settings.
目的是评估基于空间惩罚的体素内不相干运动(IVIM)方法与传统双指数(BE)模型的 IVIM 方法相比的精度和可重复性。在 3 个时间点(基线,第 1 周期后和第 3 周期后)对 40 名经活检证实为骨肉瘤的患者(N=40;年龄=17.7±5.9 岁;男:女=30:10)使用 1.5T 扫描仪采集 40 名患者的 IVIM-MRI(11 个 b 值;0-800 s/mm)。在整个肿瘤和健康肌肉组织中使用 5 种方法(1)具有三参数拟合的 BE(BE),(2)具有双参数拟合的分段 BE(BESeg-2),(3)具有单参数拟合的分段 BE(BESeg-1),(4)具有自适应全变差惩罚的 BE(BE+TV)和(5)具有自适应 Huber 惩罚的 BE(BE+HPF),分别在三个时间点估计扩散系数(D),灌注系数(D*)和灌注分数(f)。在健康组织和肿瘤组织中测量了 IVIM 参数的个体内变异系数(wCV)和个体间变异系数(bCV)。为了进行精度和可重复性评估,使用 Friedman 检验后进行 Wilcoxon 符号秩(WSR)检验,对 5 种 IVIM 方法在同一扫描中的 wCV 和 bCV 进行了比较。实验结果表明,在三个时间点,与 BE 方法相比,BE+TV 和 BE+HPF 显示出显著(p<10)较低的 D 的 wCV 和 bCV(wCV:24-32%;bCV:22-31%)(wCV:38-49%;bCV:36-46%)),健康肌肉和肿瘤中的 wCV 和 bCV。BE+TV 和 BE+HPF 还显示出与 BE,BESeg-2 和 BESeg-1 方法相比,D*(wCV:89-108%;bCV:83-102%)和 f(wCV:55-60%;bCV:56-60%)的 wCV 和 bCV 明显较低(D*-wCV:102-122%;D*-bCV:98-114%和 f-wCV:96-130%;f-bCV:94-125%),在三个时间点在肿瘤和健康组织中均如此。基于空间惩罚的 IVIM 分析方法 BE+TV 和 BE+HPF 在当前临床环境中显示出较低的变异性,并且提高了精度和可重复性。