Berkut Mariya Vladimirovna, Belyaev Aleksey Mikhailovich, Galunova Tatyana Yurievna, Tyapkin Nikolay Ivanovich, Reva Sergey Aleksandrovich, Nosov Alexander Konstantinovich
Department of Oncourology, FSBI «N.N. Petrov National Medical Research Centre of Oncology» MH of RF, St. Petersburg, Russian Federation.
Oncourology Department, Leningrad Regional Clinical Hospital, St. Petersburg, Russian Federation.
Arab J Urol. 2024 Jul 3;22(4):235-242. doi: 10.1080/20905998.2024.2373399. eCollection 2024.
Standard 24-h antibiotic prophylaxis (AP) is widely employed to minimize the risk of infection complications (ICs) within 30 days following a radical cystectomy (RC). However, a considerable variety of prophylaxis protocols do not prevent a high ICs rate after surgery (37-67%). Therefore, antibiotic's type and its duration are still controversial for AP.(.
To compare standard 24-h AP with a prolonged 120-h regimen in a multicenter randomized clinical trial.
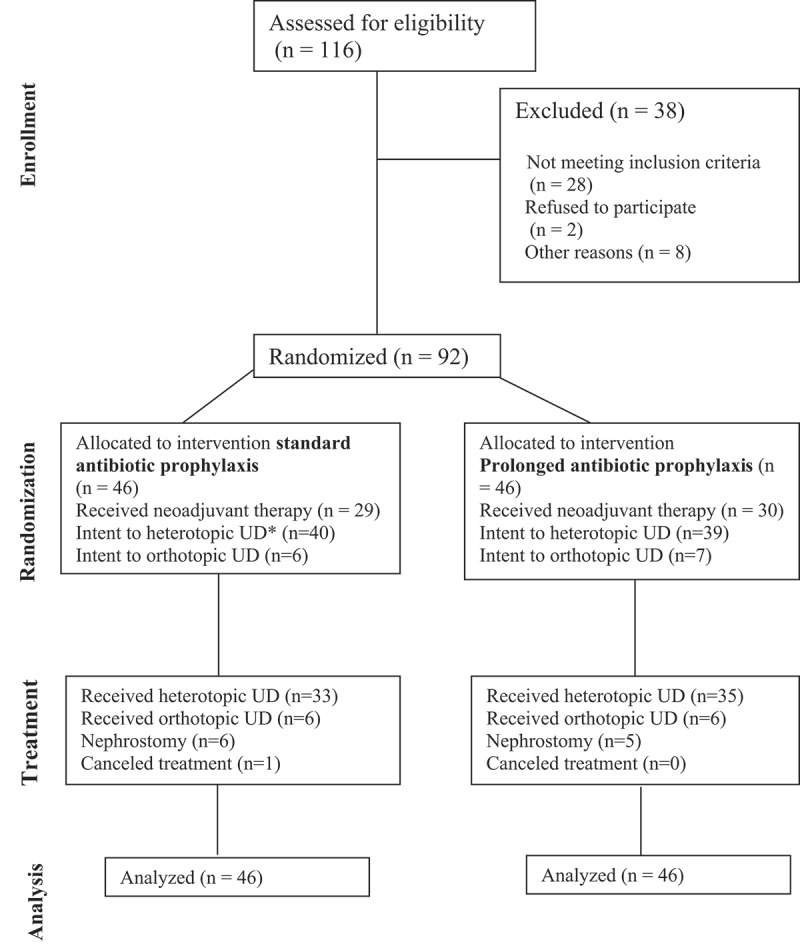
Patients were randomized in a 1:1 ratio to standard 24-h AP regimen (Group A) versus the prolonged meropenem AP 120-h (Group B). The primary endpoint was an event rate defined as the frequency of ICs within 30 days. The secondary endpoint were biomarker's analysis and antibiotic re-administration rate (ArAR).
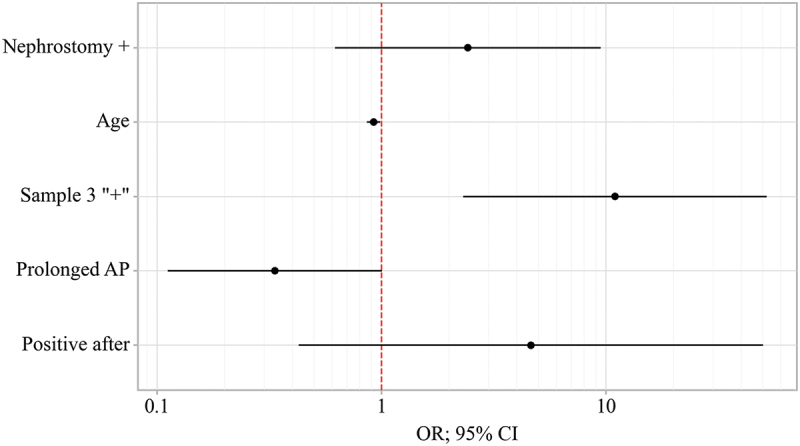
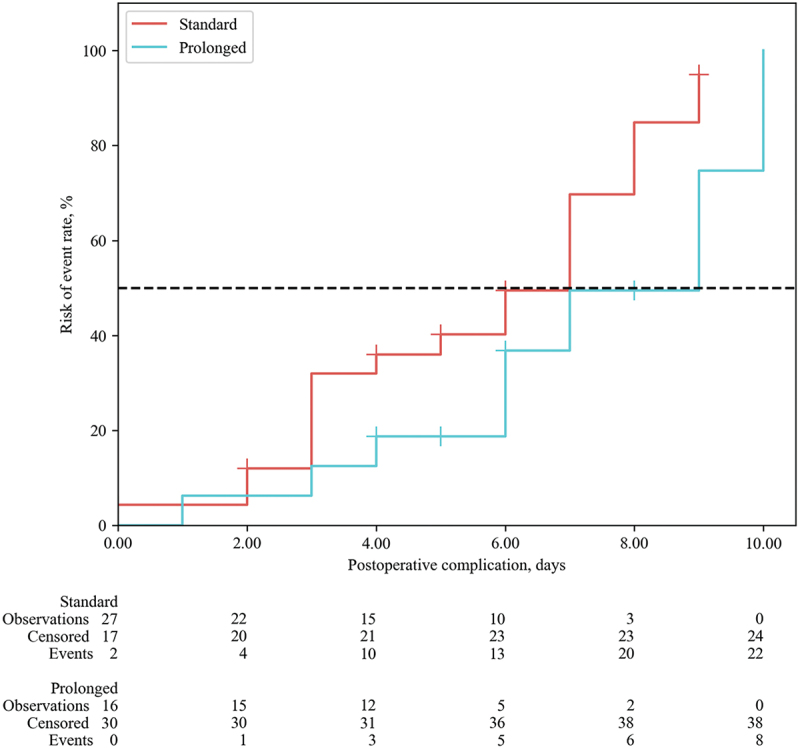
A total of 92 patients were enrolled. The Clavien-Dindo complications rate did not differ between the groups (p = 0.065), however the overall complication rate was higher in Group A (63.0% vs. 34.8%, p = 0.007). The infection complication rate was 2.75 times higher in the standard antibiotic prophylaxis group: 47.8% compared to 17.4% cases in Group B (p = 0.002). The new prolonged antibiotic regimen decreased the risk of ICs (OR 0.23; 95% CI 0.08-.598; p = 0.003).The for ICs of clinical interest in group A was 7.00 days and in group B was 9.00 days (HR = 0.447; 0.191-1.050, p = 0.065). The ArAR was higher in Group A -47.8%, while in Group B it was only in 17.4% of the cases. The incidence of bacteriuria before RC was the same between groups (p = 0.666), however, after stent removal the risk of a positive culture was lower in group B (RR = 0.64; 95% CI 0.37-1.08; p = 0.05).
The administration AP over 120-h appears to be safe and feasible, demonstrating a reduction in the total number of complications and ArAR. Trial registration in Clinical Trials: NCT05392634. NCT05392634.
标准的24小时抗生素预防(AP)被广泛应用于将根治性膀胱切除术(RC)后30天内感染并发症(ICs)的风险降至最低。然而,相当多种类的预防方案并不能防止术后出现高ICs发生率(37%-67%)。因此,抗生素的类型及其持续时间在AP中仍存在争议。
在一项多中心随机临床试验中比较标准的24小时AP与延长至120小时的方案。
患者按1:1比例随机分为标准24小时AP方案组(A组)和延长至120小时的美罗培南AP组(B组)。主要终点是定义为30天内ICs发生频率的事件发生率。次要终点是生物标志物分析和抗生素再次给药率(ArAR)。
共纳入92例患者。两组间Clavien-Dindo并发症发生率无差异(p = 0.065),但A组的总体并发症发生率更高(63.0%对34.8%,p = 0.007)。标准抗生素预防组的感染并发症发生率高2.75倍:A组为47.8%,而B组为17.4%(p = 0.002)。新的延长抗生素方案降低了ICs风险(OR 0.23;95%CI 0.08-0.598;p = 0.003)。A组临床关注的ICs持续时间为7.00天,B组为9.00天(HR = 0.447;0.191-1.050,p = 0.065)。A组的ArAR更高,为47.8%,而B组仅为17.4%的病例。RC前菌尿症的发生率在两组间相同(p = 0.666),然而,在拔除支架后,B组培养阳性的风险较低(RR = 0.64;95%CI 0.37-1.08;p = 0.05)。
超过120小时的AP给药似乎是安全可行的,显示出并发症总数和ArAR有所降低。临床试验注册:NCT05392634。NCT05392634。