Huls Gerwin, Chitu Dana A, Tick Lidwine, Boersma Rinske, Breems Dimitri, Herbers Alexandra, Klein Saskia K, de Jonge Suzan, Westerweel Peter E, Cruijsen Marjan, Hoogendoorn Mels, Cuijpers Marlous, Deeren Dries, Bailly Benjamin, Visser Otto, van Rhenen Anna, Posthuma Eduard F M, Valk Peter J M, Cloos Jacqueline, Ammatuna Emanuele, Refos Jeannine M, Fakkert R, Löwenberg Bob, Ossenkoppele Gert J
Department of Hematology, University Medical Center Groningen, PO Box 30.001, Groningen, 9700 RB, The Netherlands.
Department of Hematology, Hemato Oncology Foundation for Adults in the Netherlands, Rotterdam, The Netherlands.
Ann Hematol. 2025 Jan;104(1):361-368. doi: 10.1007/s00277-024-06033-y. Epub 2024 Oct 5.
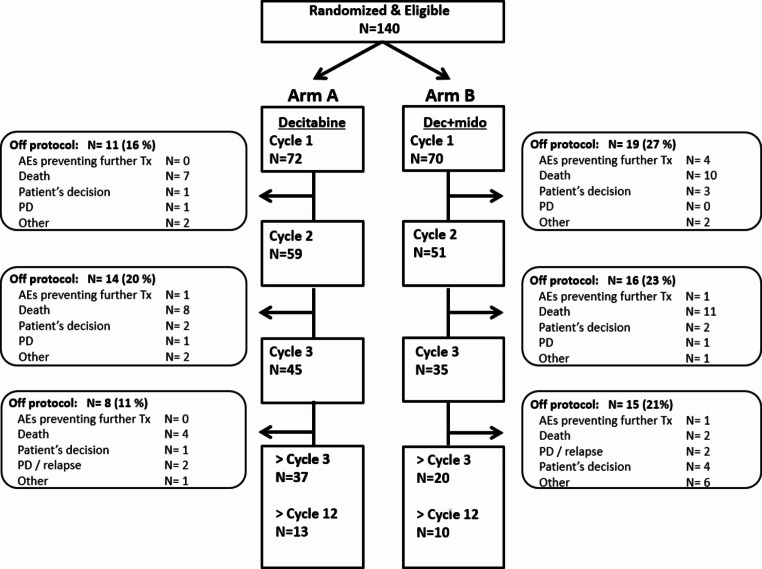
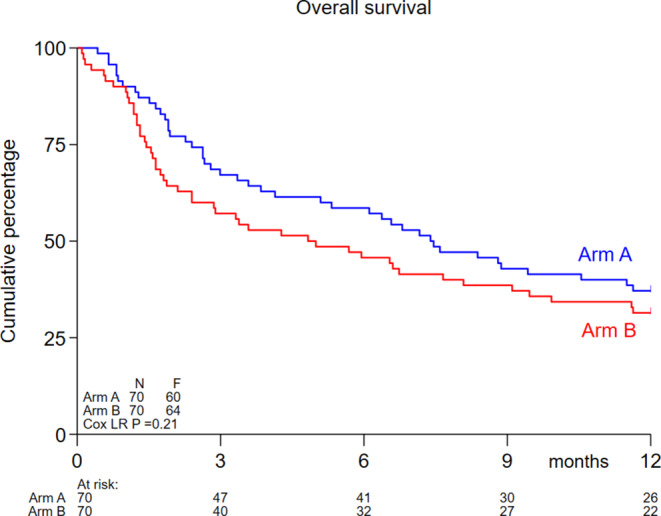
The treatment of older patients with acute myeloid leukemia (AML) considered unfit for receiving intensive chemotherapy is challenging. Based on the hypothesis that addition of the broad tyrosine kinase inhibitor (TKI) midostaurin could improve the response to hypomethylating agents, irrespective of FLT3 gene mutational status, we conducted a randomized phase II multicenter study to assess the tolerability and efficacy of the addition of midostaurin to a 10-day schedule of decitabine in unfit (i.e. Hematopoietic Cell Transplantation Comorbidity Index (HCT-CI) ≥ 3) AML and higher risk myelodysplasia (MDS) patients (HOVON155 trial). In total, 140 eligible patients were randomly (1:1) assigned to treatment with 10-days of decitabine alone (N = 70) or combined with midostaurin (50 mg bid;starting the day following the last dose of decitabine), (N = 70). Addition of midostaurin was well tolerated and the number of AEs was comparable for both treatment arms. Early death rates (< 30 days) were similar as well (10%). In the decitabine plus midostaurin arm 24% reached CR/CRi, the median OS was 4.8 months and 1-yrs OS was 31% which compared with 34% CR/CRi, median OS of 7.4 months and 1-yrs OS of 37% for the decitabine alone group (NS). Thus, while the addition of midostaurin appears safe, it does not enhance therapeutic efficacy of decitabine in unfit AML patients.
对于那些被认为不适合接受强化化疗的老年急性髓系白血病(AML)患者,其治疗颇具挑战性。基于这样一种假设,即无论FLT3基因突变状态如何,添加广谱酪氨酸激酶抑制剂(TKI)米哚妥林都可以改善对去甲基化药物的反应,我们开展了一项随机II期多中心研究,以评估在不适合(即造血细胞移植合并症指数(HCT-CI)≥3)的AML和高危骨髓增生异常综合征(MDS)患者中,将米哚妥林添加到为期10天的地西他滨治疗方案中的耐受性和疗效(HOVON155试验)。总共140名符合条件的患者被随机(1:1)分配接受单独10天地西他滨治疗(N = 70)或联合米哚妥林治疗(50 mg,每日两次;在地西他滨最后一剂后的次日开始)(N = 70)。添加米哚妥林的耐受性良好,两个治疗组的不良事件数量相当。早期死亡率(<30天)也相似(10%)。在地西他滨加米哚妥林组中,24%达到完全缓解/血细胞计数不完全恢复的完全缓解(CR/CRi),中位总生存期为4.8个月,1年总生存率为31%,而单独地西他滨组的CR/CRi为34%,中位总生存期为7.4个月,1年总生存率为37%(无显著性差异)。因此,虽然添加米哚妥林似乎是安全的,但它并不能提高地西他滨对不适合的AML患者的治疗效果。