Scholfield Daniel W, Williamson Andrew J, Cunning Nina, Awad Zaid
Department of Otolaryngology Head and Neck Surgery, Imperial College Healthcare, NHS Trust, London, W6 8RF, UK.
Department of Surgery and Cancer, Imperial College London, London, UK.
Eur Arch Otorhinolaryngol. 2025 Feb;282(2):1027-1040. doi: 10.1007/s00405-024-08976-4. Epub 2024 Oct 4.
Tongue base mucosectomy (TBM) is a well-established procedure in investigating cervical squamous cell carcinoma of occult primary. However, its risks have not been balanced against its benefits with validated tools.
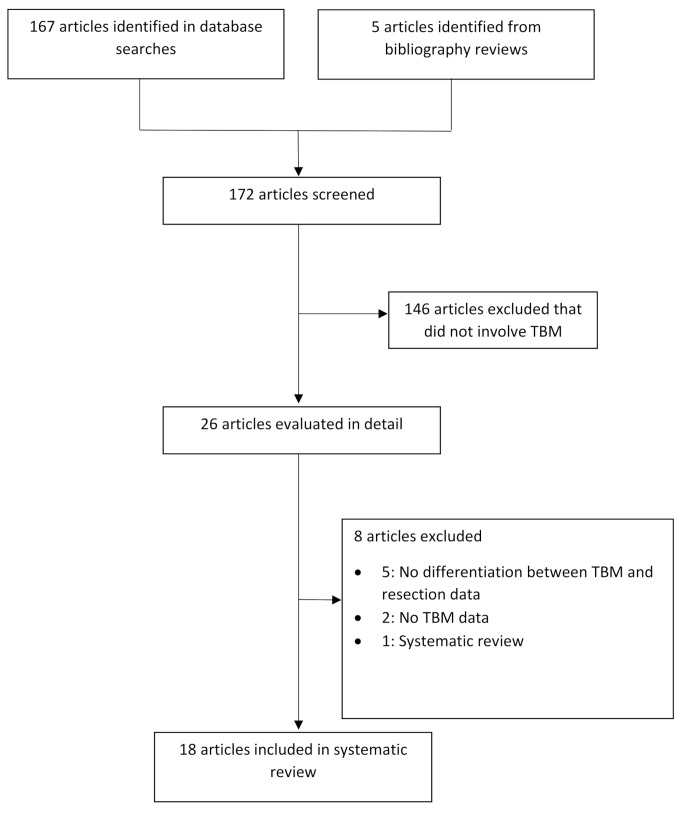
A systematic literature review was conducted for reported complications and quality-of-life outcomes following TBM. The complications and quality-of-life outcomes following TBM at our institution are then reported using objective metrics and validated assessment tools, including Performance Status Scale for Head and Neck Cancer Patients (PSS-HNS), University of Washington Quality-of-life Questionnaire (UW-QOL) and M. D. Anderson Dysphagia Inventory (MDADI).
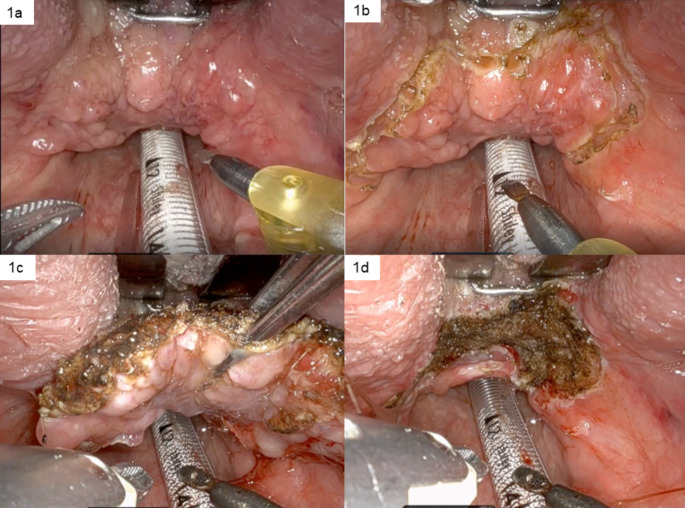
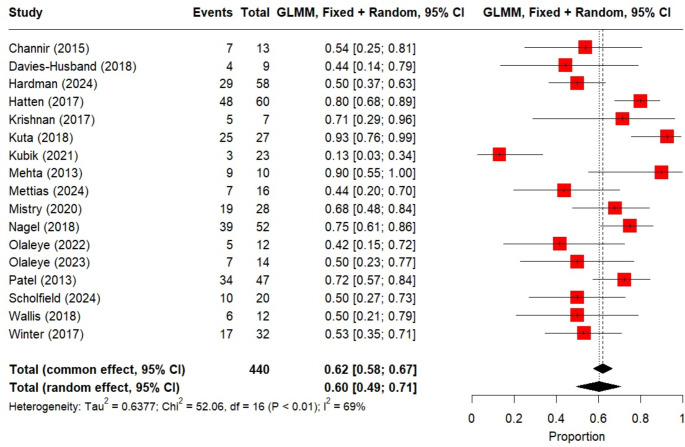
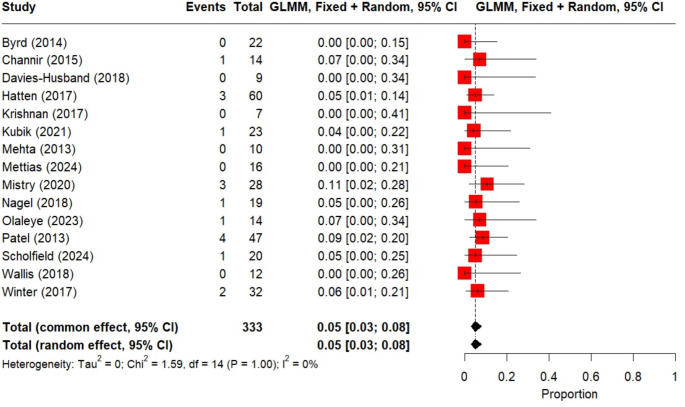
Eighteen studies met the criteria for inclusion in the systematic review. Of these, 9 addressed swallowing outcomes described in text, without using validated assessment tools. No studies reported taste, speech and pain outcomes after TBM. Post-operative bleeding was not consistently reported. 20 patients underwent robotic TBM at our institution between 2017 and 2023. The primary tumour was identified in 50% (10/20) of cases. The median time to commencing soft diet and median time of NG feeding was 0 days. The median return to normalcy of diet score was 95. Median post-treatment UW-QOL pain and swallowing scores were 100 and 70 respectively. The median speech score was 100, saliva 70, and taste 70. The median normalised MDADI scores were: global 80; emotional 67; functional 80 and physical 65.
Validated assessment tools better inform patients about treatment options and can help compare post-TBM results across institutions. Our data demonstrates that TBM patients have a functional post-operative swallow, are pain and gastrostomy free, even after adjuvant treatment. Routine post-operative insertion of NG tube is not necessary.
舌根黏膜切除术(TBM)是一种用于隐匿性原发性宫颈鳞状细胞癌研究的成熟手术。然而,其风险与益处尚未通过经过验证的工具进行权衡。
对TBM术后报告的并发症和生活质量结果进行系统的文献综述。然后使用客观指标和经过验证的评估工具,包括头颈癌患者性能状态量表(PSS-HNS)、华盛顿大学生活质量问卷(UW-QOL)和MD安德森吞咽障碍量表(MDADI),报告我们机构TBM术后的并发症和生活质量结果。
18项研究符合纳入系统评价的标准。其中,9项研究在文本中描述了吞咽结果,但未使用经过验证的评估工具。没有研究报告TBM术后的味觉、言语和疼痛结果。术后出血情况报告不一。2017年至2023年期间,我们机构有20例患者接受了机器人辅助TBM手术。50%(10/20)的病例中发现了原发性肿瘤。开始软食的中位时间和鼻饲的中位时间均为0天。饮食评分恢复正常的中位时间为95天。治疗后UW-QOL疼痛和吞咽评分的中位数分别为100和70。言语评分中位数为100,唾液评分中位数为70,味觉评分中位数为70。MDADI标准化评分的中位数为:总体80;情感67;功能80;身体65。
经过验证的评估工具能更好地让患者了解治疗选择,并有助于比较不同机构TBM术后的结果。我们的数据表明,TBM患者术后吞咽功能良好,即使在辅助治疗后也没有疼痛且无需胃造口术。术后常规插入鼻胃管没有必要。