Sivagnanam Harish, Senthilkumar P K, Velu Kannan Bhaba, Anand Murugesh, Viswanathan Ramasubramanian
Department of Nephrology, Tirunelveli Medical College and Hospital, Tirunelveli, Tamil Nadu, India.
Indian J Nephrol. 2024 Sep-Oct;34(5):453-460. doi: 10.4103/ijn.ijn_57_23. Epub 2023 Oct 23.
Patients with chronic kidney disease have muscle wasting, sarcopenia, and cachexia that contribute to frailty and morbidity. The present study assessed the prevalence of protein-energy wasting in dialysis-dependent chronic kidney disease population and evaluated the validity of various nutritional assessment tools in diagnosing protein-energy wasting.
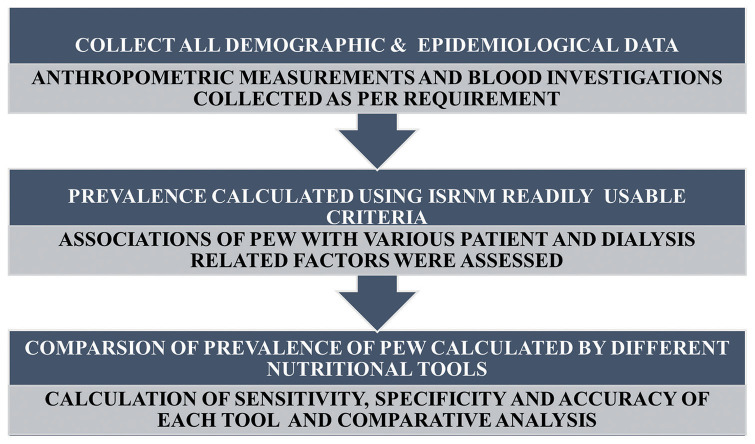
All patients above 18 years undergoing dialysis for more than 3 months without any active infection or malignancy were included in our study. Data from anthropometric measurements, dietary assessment, and blood investigations were collected. Protein-energy wasting was assessed by the International Society of Renal Nutrition and Metabolism 2008 criteria. Diagnostic validity of the nutritional assessment tools to predict protein-energy wasting was estimated by area under the curve, sensitivity, specificity, and accuracy statistics.
A total of 146 patients were studied. The prevalence of protein-energy wasting was 56.8%. Protein-energy wasting was significantly associated with socioeconomic status, hospitalization days, and catheter days. Normalized protein catabolism rate had the highest sensitivity (90.4%) for predicting protein-energy wasting. Malnutritional inflammatory score had the highest area under the curve (0.858), specificity (82.5%), and accuracy (82.2%). Mid-upper arm circumference, Dialysis Malnutrition Score, and albumin were also found to be significant predictors of protein-energy wasting.
Lack of advanced equipment in suburban and rural centers to detect protein-energy wasting in India can be overcome by using the various stand-alone and combination nutrition assessment tools which have been validated in the present study.
慢性肾脏病患者存在肌肉萎缩、肌肉减少症和恶病质,这些会导致身体虚弱和发病。本研究评估了依赖透析的慢性肾脏病患者中蛋白质能量消耗的患病率,并评估了各种营养评估工具在诊断蛋白质能量消耗方面的有效性。
纳入所有年龄在18岁以上、接受透析超过3个月且无任何活动性感染或恶性肿瘤的患者。收集人体测量、饮食评估和血液检查的数据。根据国际肾脏营养与代谢学会2008年标准评估蛋白质能量消耗。通过曲线下面积、敏感性、特异性和准确性统计来估计营养评估工具预测蛋白质能量消耗的诊断有效性。
共研究了146例患者。蛋白质能量消耗的患病率为56.8%。蛋白质能量消耗与社会经济状况、住院天数和置管天数显著相关。标准化蛋白质分解代谢率预测蛋白质能量消耗的敏感性最高(90.4%)。营养不良炎症评分的曲线下面积最大(0.858),特异性最高(82.5%),准确性最高(82.2%)。上臂中部周长、透析营养不良评分和白蛋白也被发现是蛋白质能量消耗的重要预测指标。
在印度,通过使用本研究中已验证的各种单独和联合营养评估工具,可以克服城乡中心缺乏先进设备来检测蛋白质能量消耗的问题。