Vigneron Clara, Devautour Clément, Charpentier Julien, Birsen Rudy, Jamme Matthieu, Pène Frédéric
Service de Médecine Intensive-Réanimation, Hôpital Cochin, Assistance Publique - Hôpitaux de Paris, 27 rue du Faubourg Saint Jacques, Paris, 75014, France.
Université Paris Cité, Paris, France.
Ann Intensive Care. 2024 Oct 7;14(1):155. doi: 10.1186/s13613-024-01383-2.
Bleeding events are common complications in critically ill patients with haematological malignancies. The objective of this study was to assess the incidence and identify determinants of ICU-acquired severe bleeding events in critically ill patients with haematological malignancies. We conducted a single-center retrospective study including all adult patients with a history of haematological malignancy requiring unplanned ICU admission over a 12-year period (2007-2018). The primary endpoint was the occurrence of ICU-acquired (i.e. after the first 24 h in the ICU) severe bleeding events, as defined as grades 3 or 4 of the World Health Organization classification.
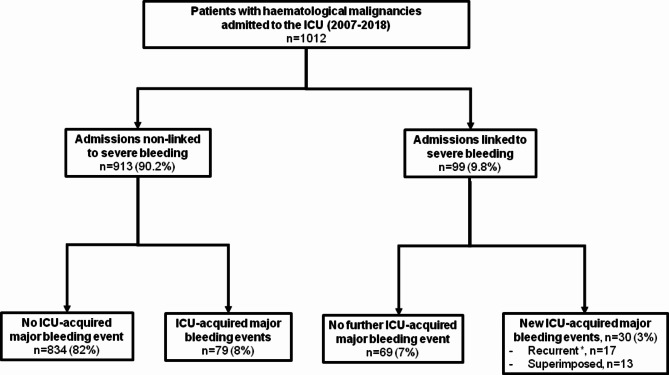
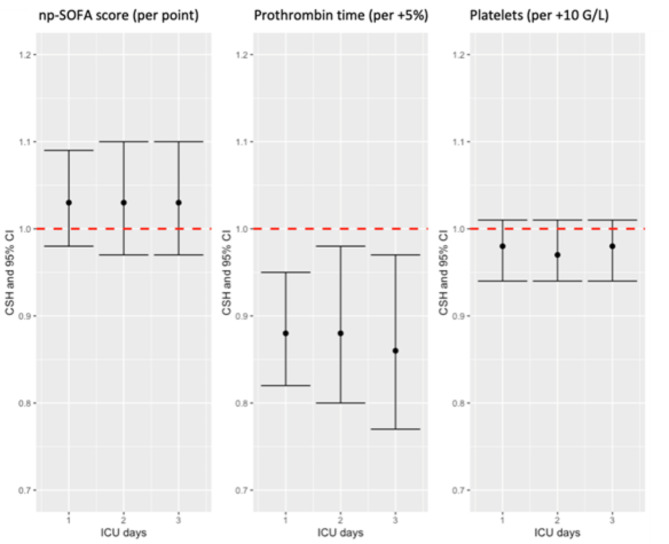
A total of 1012 patients were analysed, mainly with a diagnosis of lymphoma (n = 434, 42.9%) and leukaemia or myelodysplastic syndrome (n = 266, 26.3%). Most patients were recently diagnosed (n = 340, 33.6%) and under active cancer treatment within the last 3 months (n = 604, 59.7%). The main cause for admission was infection (n = 479, 47.3%), but a significant proportion of patients were admitted for a primary haemorrhage (n = 99, 10%). ICU-acquired severe bleeding events occurred in 109 (10.8%) patients after 3.0 days [1.0-7.0] in the ICU. The main source of bleeding was the gastrointestinal tract (n = 44, 40.3%). Patients experiencing an ICU-acquired severe bleeding event displayed prolonged in-ICU length of stay (9.0 days [1.0-6.0] vs. 3.0 [3.5-15.0] in non-bleeding patients, p < 0.001) and worsened outcomes with increased in-ICU and in-hospital mortality rates (55% vs. 18.3% and 65.7% vs. 33.1%, respectively, p < 0.001). In multivariate analysis, independent predictors of ICU-acquired severe bleeding events were chronic kidney disease (cause-specific hazard 2.00 [1.19-3.31], p = 0.008), a primary bleeding event present at the time of ICU admission (CSH 4.17 [2.71-6.43], p < 0.001), non-platelet SOFA score (CSH per point increase 1.06 [1.01-1.11], p = 0.02) and prolonged prothrombin time (CSH per 5-percent increase 0.90 [0.85-0.96], p = 0.001) on the day prior to the event of interest.
Major bleeding events are common complications in critically ill patients with haematological malignancies and are associated with a worsened prognosis. We identified relevant risk factors of bleeding which may prompt closer monitoring or preventive measures.
出血事件是血液系统恶性肿瘤重症患者常见的并发症。本研究的目的是评估血液系统恶性肿瘤重症患者发生重症监护病房(ICU)获得性严重出血事件的发生率,并确定其决定因素。我们进行了一项单中心回顾性研究,纳入了12年间(2007 - 2018年)所有有血液系统恶性肿瘤病史且需要非计划入住ICU的成年患者。主要终点是ICU获得性(即入住ICU 24小时后)严重出血事件的发生情况,按照世界卫生组织分类标准定义为3级或4级。
共分析了1012例患者,主要诊断为淋巴瘤(n = 434,42.9%)以及白血病或骨髓增生异常综合征(n = 266,26.3%)。大多数患者为近期确诊(n = 340,33.6%)且在过去3个月内正在接受积极的癌症治疗(n = 604,59.7%)。入院的主要原因是感染(n = 479,47.3%),但有相当比例的患者因原发性出血入院(n = 99,10%)。109例(10.8%)患者在入住ICU 3.0天[1.0 - 7.0]后发生了ICU获得性严重出血事件。出血的主要来源是胃肠道(n = 44,40.3%)。发生ICU获得性严重出血事件的患者ICU住院时间延长(出血患者为9.0天[1.0 - 6.0],非出血患者为3.0天[3.5 - 15.0],p < 0.001),且ICU和院内死亡率增加,预后恶化(分别为55%对18.3%和65.7%对33.1%,p < 0.001)。在多变量分析中,ICU获得性严重出血事件的独立预测因素为慢性肾脏病(病因特异性风险2.00 [1.19 - 3.31],p = 0.008)、入住ICU时存在原发性出血事件(CSH 4.17 [2.71 - 6.43],p < 0.001)、非血小板序贯器官衰竭评估(SOFA)评分(每增加1分CSH 1.06 [1.01 - 1.11],p = 0.02)以及在感兴趣事件发生前一天凝血酶原时间延长(每增加5% CSH 0.90 [0.85 - 0.96],p = 0.001)。
大出血事件是血液系统恶性肿瘤重症患者常见的并发症,且与预后恶化相关。我们确定了出血的相关危险因素,这可能促使进行更密切的监测或采取预防措施。