Kapur Akshat, Rojas-Anaya Héctor, Roberts Graham, Roland Damian, Gupta Atul, Lazner Michaela, Bayreuther Jane, Cantle Fleur, Jones Christina, Pappachan John, Bremner Stephen, James David, Fitzgerald Shane, Owens Kelly, Asim Lalarukh, Khaleva Ekaterina, Seddon Paul
University Hospitals Sussex NHS Foundation Trust, Brighton, UK.
Brighton and Sussex Clinical Trials Unit, Brighton, UK.
ERJ Open Res. 2024 Oct 7;10(5). doi: 10.1183/23120541.00168-2024. eCollection 2024 Sep.
Treating children with acute severe asthma (ASA) who fail to respond to first-line inhaled bronchodilators is problematic: use of intravenous agents is inconsistent and side-effects are common. High-flow humidified oxygen (HiFlo) has shown promise in other respiratory conditions and is increasingly used in ASA, but with little evidence.
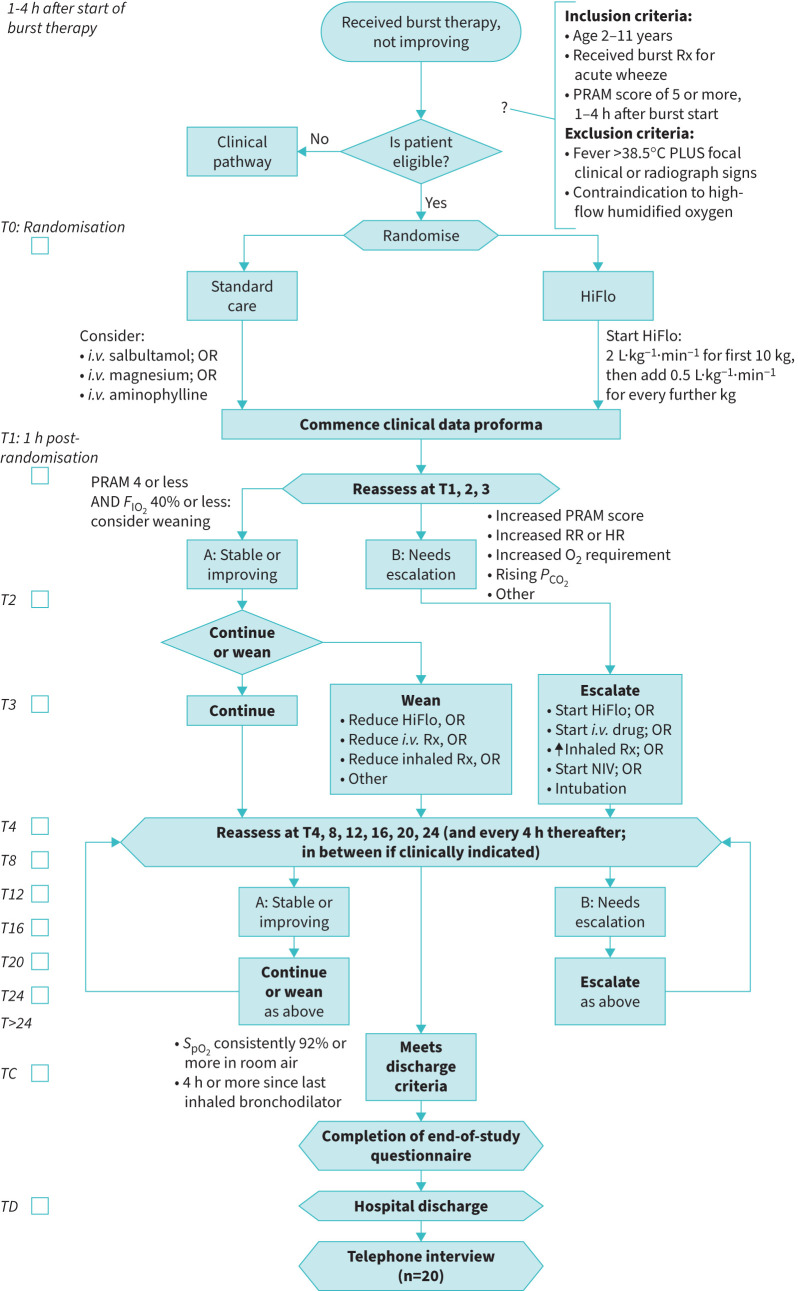
We conducted a feasibility randomised controlled trial with deferred consent to assess early HiFlo in children aged 2-11 years with ASA not responding to "burst" therapy (high-dose inhaled salbutamol ± ipratropium). Children with Paediatric Respiratory Assessment Measure (PRAM) score 5+ after "burst" were randomised to commence HiFlo or follow standard care. Candidate primary outcomes assessed were treatment failure requiring escalation, and time to meeting hospital discharge criteria.
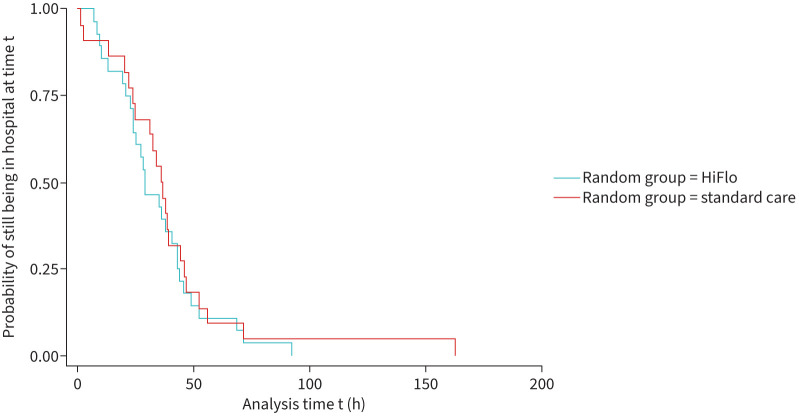
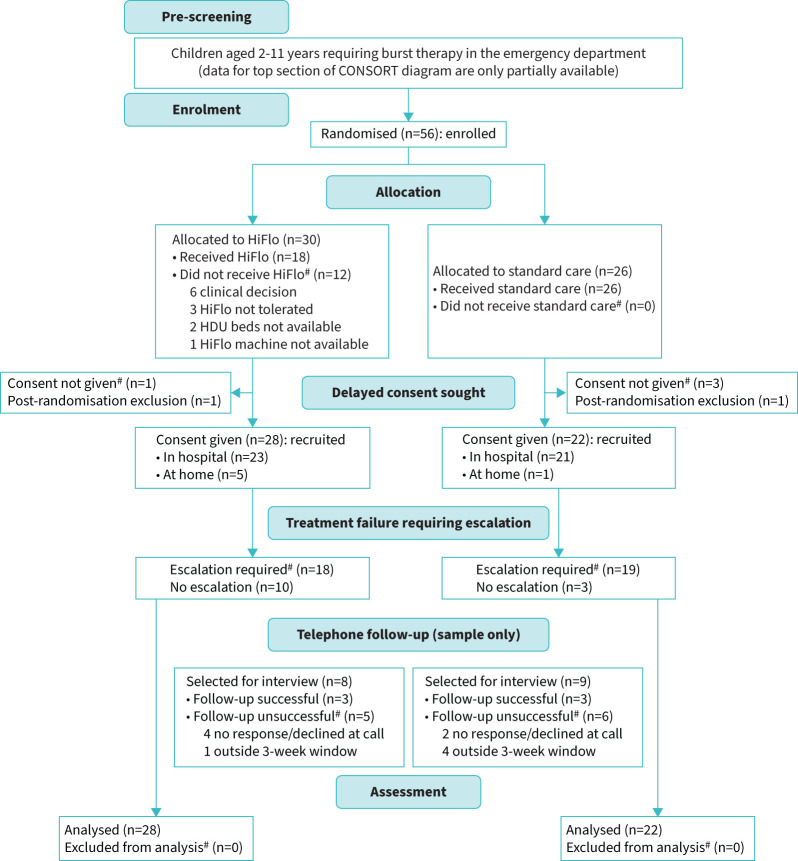
The target was met despite coronavirus disease 2019 pandemic disruption: 56 children were randomised across four sites, with deferred consent received in 50 out of 56 (89%), and mean recruitment rate 1.1 per site per month. 28 were allocated early HiFlo and 22 standard care. Data collection was complete for both candidate primary outcomes. Treatment failure requiring escalation occurred in 18 of 28 children (64%) in the HiFlo arm and in 19 of 22 (86%) in the standard care arm. Median (interquartile range) time from randomisation to meeting discharge criteria was 29.3 h (21.8-43.7 h) in the HiFlo arm and 36.8 h (24.1-46.3 h) in the standard care arm.
HiFlo in childhood ASA is a potentially promising intervention whose use is increasing despite lack of evidence. A definitive randomised controlled trial to assess its effectiveness is required and appears to be feasible.
对于一线吸入性支气管扩张剂治疗无效的急性重度哮喘(ASA)患儿,治疗存在问题:静脉用药方法不一致且副作用常见。高流量湿化氧(HiFlo)在其他呼吸道疾病中已显示出前景,并且在ASA治疗中使用越来越多,但证据很少。
我们进行了一项可行性随机对照试验,并采用延迟同意的方式,以评估早期使用HiFlo对2至11岁、接受“冲击”治疗(高剂量吸入沙丁胺醇±异丙托溴铵)无效的ASA患儿的疗效。“冲击”治疗后儿科呼吸评估量表(PRAM)评分为5分及以上的患儿被随机分组,开始使用HiFlo或遵循标准治疗。评估的主要候选结局为需要升级治疗的治疗失败情况,以及达到出院标准的时间。
尽管受到2019年冠状病毒病大流行的干扰,但仍达到了目标:56名患儿在四个地点进行了随机分组,56名中有50名(89%)获得了延迟同意,平均每个地点每月招募率为1.1名。28名被分配接受早期HiFlo治疗,22名接受标准治疗。两个主要候选结局的数据收集均已完成。HiFlo组28名患儿中有18名(64%)出现需要升级治疗的治疗失败情况,标准治疗组22名患儿中有19名(86%)出现这种情况。HiFlo组从随机分组到达到出院标准的中位(四分位间距)时间为29.3小时(21.8 - 43.7小时),标准治疗组为36.8小时(24.1 - 46.3小时)。
儿童ASA使用HiFlo是一种潜在有前景的干预措施,尽管缺乏证据,但其使用仍在增加。需要进行一项确定性随机对照试验来评估其有效性,且这似乎是可行的。