Ott Johannes, Robin Geoffroy, Hager Marlene, Dewailly Didier
Clinical Division of Gynecological Endocrinology and Reproductive Medicine, Department of Obstetrics and Gynecology, Medical University of Vienna, Vienna, Austria.
Reproductive Endocrinology Unit, Lille University Hospital, Lille, France.
Hum Reprod Update. 2025 Jan 1;31(1):64-79. doi: 10.1093/humupd/dmae030.
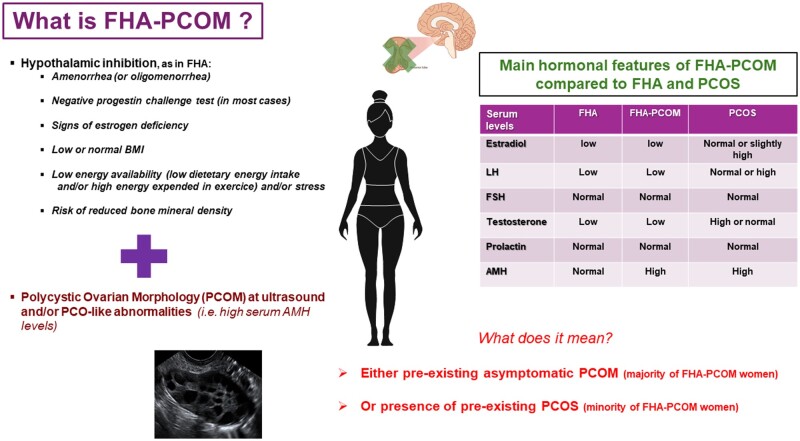
Functional hypothalamic amenorrhoea (FHA) is responsible for 20-35% of all cases of secondary amenorrhoea and, thus, is the second most common cause of secondary amenorrhoea after polycystic ovary syndrome (PCOS). A high number of patients with FHA reveal polycystic ovarian morphology (PCOM) on ultrasound. The combination of amenorrhoea and PCOM can lead to confusion. First, amenorrhoeic women with PCOM fulfil the revised Rotterdam criteria and, thus, can easily be misdiagnosed with PCOS. Moreover, it has been claimed that some women with FHA and concomitant PCOM differ from those without PCOM in terms of endocrine regulation and metabolic traits.
The main focus of this article was on studies about FHA, which differentiated between patients with or without PCOM. The aim was to estimate the prevalence of PCOM and to look if it has an impact on pathophysiologic, diagnostic and therapeutic issues as well as on long-term consequences.
Peer review original and review articles were selected from PubMed searches for this review. Searches were performed using the search terms 'polycystic AND functional hypothalamic amenorrhoea'. The reference lists of publications found were searched for relevant additional studies. The inclusion criteria for publications were: English language, patients' age ≥ 18 years, year of publication >1980, original studies, validated diagnosis of FHA, and validated diagnosis of PCOM using transvaginal ultrasound.
The prevalence of PCOM in women with FHA varied from 41.9% to 46.7%, which is higher than in healthy non-PCOS controls. Hypothetically, the high prevalence might be due to a mixture of silent PCOM, as in the general population, and pre-existing PCOS. Several differences in metabolic and hormonal parameters were found between FHA-PCOM and FHA-non-PCOM patients. While oestrogen deficiency is common to both groups of patients, FHA-PCOM patients have a higher BMI, higher levels of anti-Müllerian hormone (AMH) and testosterone, a higher increase in LH in the course of a GnRH test, and lower sex hormone binding globulin (SHBG) levels than FHA-non-PCOM patients. The differential diagnosis between FHA-PCOM and PCOS, especially PCOS phenotype D (PCOM and oligo-/anovulation without hyperandrogenism), can be challenging. Several parameters have been suggested, which are helpful though not absolutely reliable. They include the typical causes for FHA (excessive exercise, energy deficit, and/or psychological stress), the serum levels of LH, testosterone, and SHBG, as well as the progestin challenge test. Whether FHA-PCOM has a different risk profile for long-term consequences concerning patients' metabolic and cardiovascular situation as well as their bone mass, is unclear. Concerning therapeutic aspects, there are only few data about FHA-PCOM compared to FHA-non-PCOM. To treat anovulation, the use of pulsatile GnRH treatment seems to be equally effective in both groups. Similar to FHA-non-PCOM patients, pulsatile GnRH therapy would be more efficient than exogenous gonadotropins in FHA-PCOM patients.
Women with FHA-PCOM present a special sub-population of FHA patients. The diagnostic pitfall of FHA-PCOM should be emphasized in clinical guidelines about FHA and PCOS. The fact that almost half of the women with FHA have an ovarian follicle excess (i.e. PCOM) in face of low gonadotropin serum levels suggests that the intra-ovarian regulation of folliculogenesis is subject to individual variations, for unknown reasons, either genetic or epigenetic. Further studies are needed to investigate this hypothesis.
Not applicable.
功能性下丘脑性闭经(FHA)占所有继发性闭经病例的20% - 35%,是继多囊卵巢综合征(PCOS)之后继发性闭经的第二大常见原因。大量FHA患者在超声检查中显示多囊卵巢形态(PCOM)。闭经与PCOM的并存可能导致诊断混淆。首先,患有PCOM的闭经女性符合修订后的鹿特丹标准,因此容易被误诊为PCOS。此外,有观点认为,一些患有FHA且伴有PCOM的女性在内分泌调节和代谢特征方面与不伴有PCOM的女性有所不同。
本文主要关注关于FHA的研究,这些研究区分了有或没有PCOM的患者。目的是评估PCOM的患病率,并探讨其是否对病理生理、诊断和治疗问题以及长期后果产生影响。
从PubMed搜索中选择同行评审的原始研究和综述文章用于本综述。使用搜索词“多囊性 AND 功能性下丘脑性闭经”进行检索。对所找到出版物的参考文献列表进行搜索,以查找相关的其他研究。出版物的纳入标准为:英文、患者年龄≥18岁、出版年份>1980年、原始研究、FHA的确诊诊断以及使用经阴道超声对PCOM的确诊诊断。
FHA女性中PCOM的患病率在41.9%至46.7%之间,高于健康的非PCOS对照人群。理论上,高患病率可能是由于与普通人群一样存在隐匿性PCOM以及既往存在的PCOS共同导致的。FHA - PCOM患者与FHA - 非PCOM患者在代谢和激素参数方面存在一些差异。虽然两组患者都存在雌激素缺乏,但FHA - PCOM患者的BMI更高、抗苗勒管激素(AMH)和睾酮水平更高、GnRH试验过程中LH升高幅度更大,且性激素结合球蛋白(SHBG)水平低于FHA - 非PCOM患者。FHA - PCOM与PCOS,尤其是PCOS表型D(PCOM且伴有少排卵/无排卵但无高雄激素血症)之间的鉴别诊断可能具有挑战性。已经提出了几个参数,这些参数虽然并非绝对可靠,但有所帮助。它们包括FHA的典型病因(过度运动、能量缺乏和/或心理压力)、LH、睾酮和SHBG的血清水平以及孕激素激发试验。目前尚不清楚FHA - PCOM在患者代谢、心血管状况以及骨量等长期后果方面是否具有不同的风险特征。在治疗方面,与FHA - 非PCOM相比,关于FHA - PCOM的数据较少。对于治疗无排卵,使用脉冲式GnRH治疗在两组中似乎同样有效。与FHA - 非PCOM患者类似,脉冲式GnRH治疗在FHA - PCOM患者中比外源性促性腺激素更有效。
患有FHA - PCOM的女性是FHA患者中的一个特殊亚群。在关于FHA和PCOS的临床指南中应强调FHA - PCOM的诊断陷阱。几乎一半的FHA女性在促性腺激素血清水平较低的情况下存在卵巢卵泡过多(即PCOM)这一事实表明,卵泡发生的卵巢内调节存在个体差异,原因不明,可能是遗传或表观遗传因素。需要进一步研究来探讨这一假设。
不适用。