Roberts Surain B, Choi Woo Jin, Worobetz Lawrence, Vincent Catherine, Flemming Jennifer A, Cheung Angela, Qumosani Karim, Swain Mark, Grbic Dusanka, Ko Hin Hin, Peltekian Kevork M, Abrahamyan Lusine, Saini Monika, Tirona Kattleya, Aziz Bishoi, Lytvyak Ellina, Invernizzi Pietro, Ponsioen Cyriel Y, Bruns Tony, Cazzagon Nora, Lindor Keith, Dalekos George N, Gatselis Nikolaos K, Verhelst Xavier, Floreani Annarosa, Corpechot Christophe, Mayo Marlyn J, Levy Cynthia, Londoño Maria-Carlota, Battezzati Pier M, Pares Albert, Nevens Frederik, van der Meer Adriaan, Kowdley Kris V, Trivedi Palak J, Lleo Ana, Thorburn Douglas, Carbone Marco, Selzner Nazia, Gulamhusein Aliya F, Janssen Harry LA, Montano-Loza Aldo J, Mason Andrew L, Hirschfield Gideon M, Hansen Bettina E
Toronto Centre for Liver Disease, Toronto General Hospital, University Health Network, Toronto, Canada.
Li Ka Shing Knowledge Institute, St Michael's Hospital, Unity Health Toronto, Toronto, Canada.
JHEP Rep. 2024 Jul 8;6(10):101168. doi: 10.1016/j.jhepr.2024.101168. eCollection 2024 Oct.
BACKGROUND & AIMS: Biochemical response to ursodeoxycholic acid (UDCA) therapy is associated with good prognosis in people living with primary biliary cholangitis (PBC). Biochemical response is typically assessed early in disease and it is not known what proportion of patients lose previously attained biochemical response, nor whether this impacts long-term liver transplant (LT)-free survival.
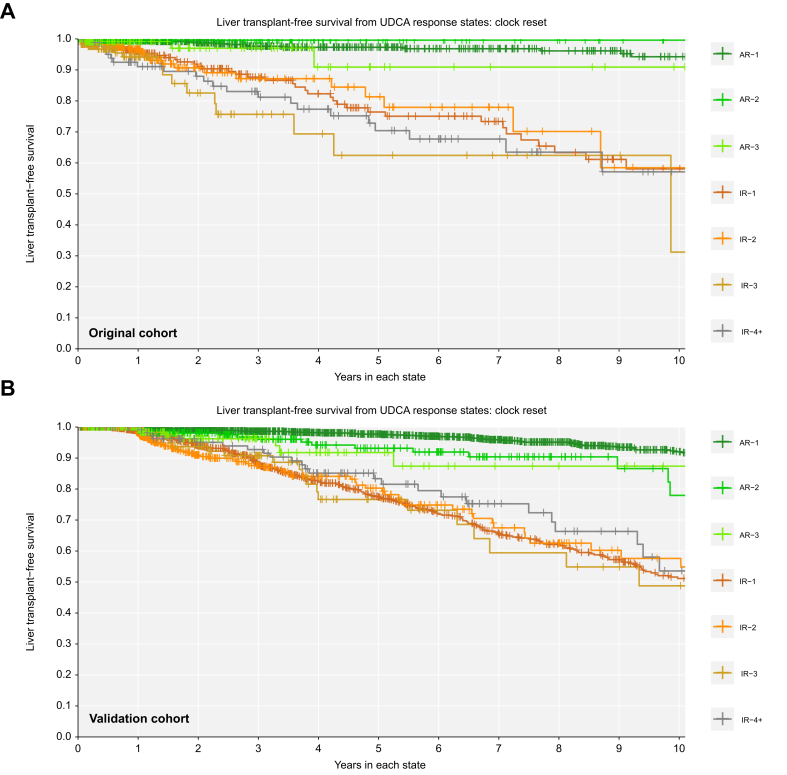
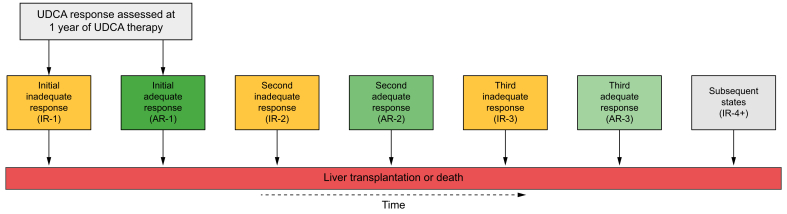
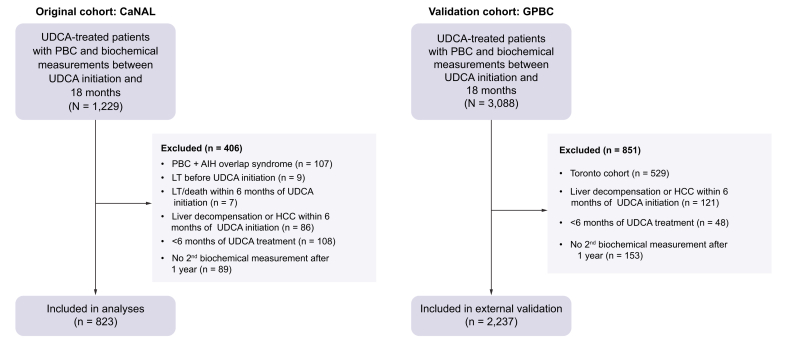
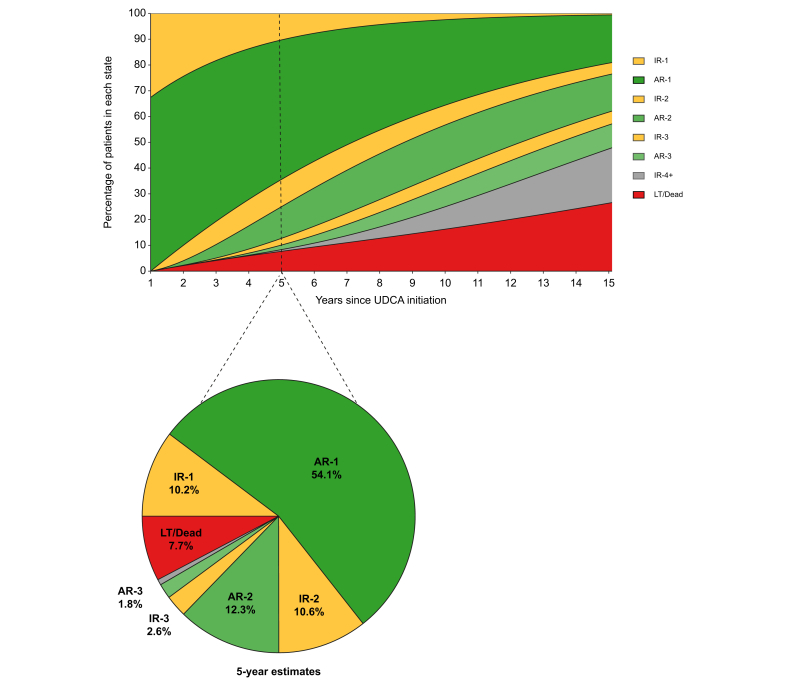
We identified all UDCA-treated patients with PBC from the Canadian Network for Autoimmune Liver disease with biochemical measurements at 1 year, and evaluated their liver biochemistry over time. Inadequate biochemical response was defined as serum alkaline phosphatase ≥1.67x the upper limit of normal or abnormal serum total bilirubin at 1 year of UDCA therapy and all time points thereafter. Multistate Markov models were used to estimate transition rates between biochemical response states and from each state to LT or death. Results were validated in an external cohort (GLOBAL PBC registry).
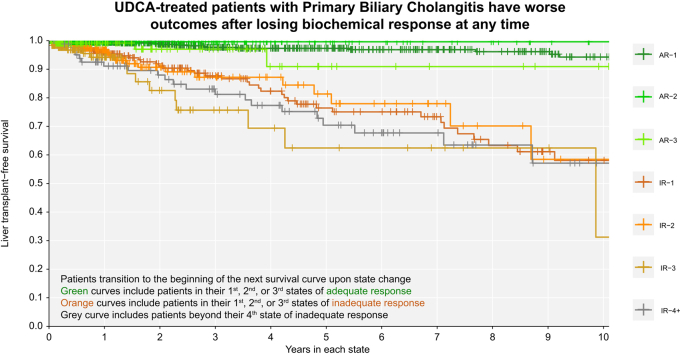
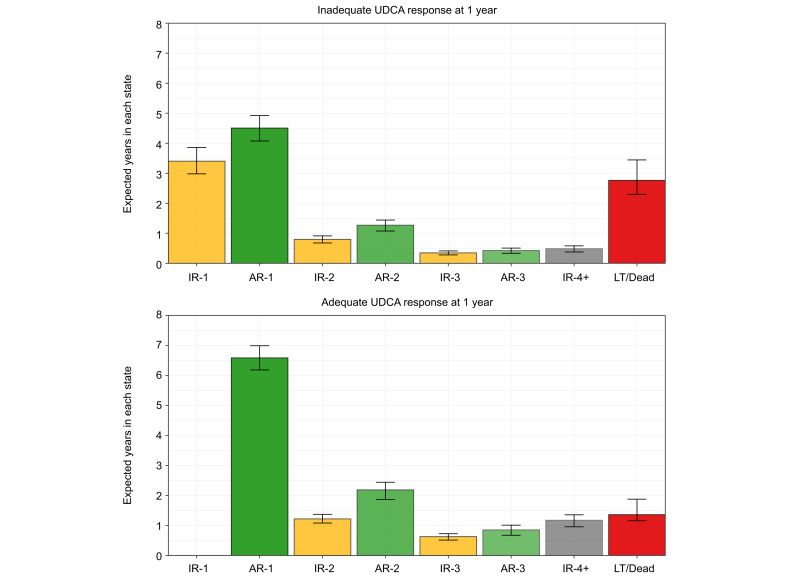
A total of 823 patients from eight centers were included. Mean age at diagnosis was 53 years, 91% were female, 33% had inadequate biochemical response to UDCA at 1 year (n = 269). Patients who retained initial adequate response had lower rates of LT or death compared to patients who subsequently lost response (relative rate 0.102, 95% CI 0.047-0.223). Patients who regained adequate response had lower rates than patients who did not (0.016, 95% CI 0.001-0.568), and patients who lost response once more (0.010, 95% CI 0.001-0.340). Patients who regained adequate response for a third time also had lower rates than patients who did not (0.151, 95% CI 0.040-0.566). Analyses in the GLOBAL PBC registry (n = 2,237) validated these results.
Loss of biochemical response at any time is associated with heightened risks of LT or death in people living with PBC. Achievement of biochemical response is an important goal throughout follow-up, regardless of biochemical response profile early in therapy.
Early biochemical response to ursodeoxycholic acid is associated with good prognosis in patients with primary biliary cholangitis (PBC). Our work demonstrates that patients with PBC transition between biochemical response states over time, and that these transitions correspond with changes in risk of liver transplantation or death. Clinicians should re-evaluate risk and optimize treatment decisions for patients with PBC throughout follow-up, regardless of early biochemical response to therapy.
原发性胆汁性胆管炎(PBC)患者对熊去氧胆酸(UDCA)治疗的生化反应与良好预后相关。生化反应通常在疾病早期进行评估,目前尚不清楚有多少患者会失去先前获得的生化反应,也不清楚这是否会影响长期无肝移植(LT)生存率。
我们从加拿大自身免疫性肝病网络中识别出所有接受UDCA治疗的PBC患者,并在1年时进行生化指标测量,然后随时间评估他们的肝脏生化指标。生化反应不充分定义为在UDCA治疗1年及此后所有时间点血清碱性磷酸酶≥正常上限的1.67倍或血清总胆红素异常。使用多状态马尔可夫模型来估计生化反应状态之间以及从每个状态到肝移植或死亡的转换率。结果在一个外部队列(全球PBC登记处)中得到验证。
共纳入来自8个中心的823例患者。诊断时的平均年龄为53岁,91%为女性,33%在1年时对UDCA的生化反应不充分(n = 269)。与随后失去反应的患者相比,保持初始充分反应的患者肝移植或死亡发生率较低(相对率0.102,95%CI 0.047 - 0.22)。恢复充分反应的患者比未恢复的患者发生率低(0.016,95%CI 0.001 - 0.568),也比再次失去反应的患者发生率低(0.010,95%CI 0.001 - 0.340)。第三次恢复充分反应的患者也比未恢复的患者发生率低(0.151,95%CI 0.040 - 0.566)。全球PBC登记处(n = 2237)的分析验证了这些结果。
在任何时候生化反应的丧失都与PBC患者肝移植或死亡风险的增加相关。实现生化反应是整个随访过程中的一个重要目标,无论治疗早期的生化反应情况如何。
原发性胆汁性胆管炎(PBC)患者对熊去氧胆酸的早期生化反应与良好预后相关。我们的研究表明,PBC患者的生化反应状态会随时间发生转变,且这些转变与肝移植或死亡风险的变化相对应。临床医生应在整个随访过程中重新评估PBC患者的风险并优化治疗决策,无论其对治疗的早期生化反应如何。