Saar Angelika, Müller Jonas, Veser Yannick, Behr Frederik, Rathmann Eiko, Schroeder Henry W S, Flöel Agnes, Müller Jan-Uwe, von Sarnowski Bettina, Fleischmann Robert
Department of Neurology, University Medicine Greifswald, Greifswald, Germany.
Department of Psychosomatics and Psychotherapy, Bethanien Hospital for Psychiatry, Greifswald, Germany.
Front Med (Lausanne). 2024 Sep 24;11:1433380. doi: 10.3389/fmed.2024.1433380. eCollection 2024.
Advances in spine surgery enable safe interventions in elderly patients, but perioperative neurocognitive disorders (pNCD), such as post-operative delirium (POD) and cognitive dysfunction (POCD), remain a serious concern. Pre-operative cognitive impairment is a major risk factor for pNCD. Comprehensive pre-operative cognitive assessments are not feasible in clinical practice, making effective screening methods desirable. This study investigates whether pre-operative cerebrovascular duplex sonography can assess subcortical (vascular) cognitive impairment and the risk for POD.
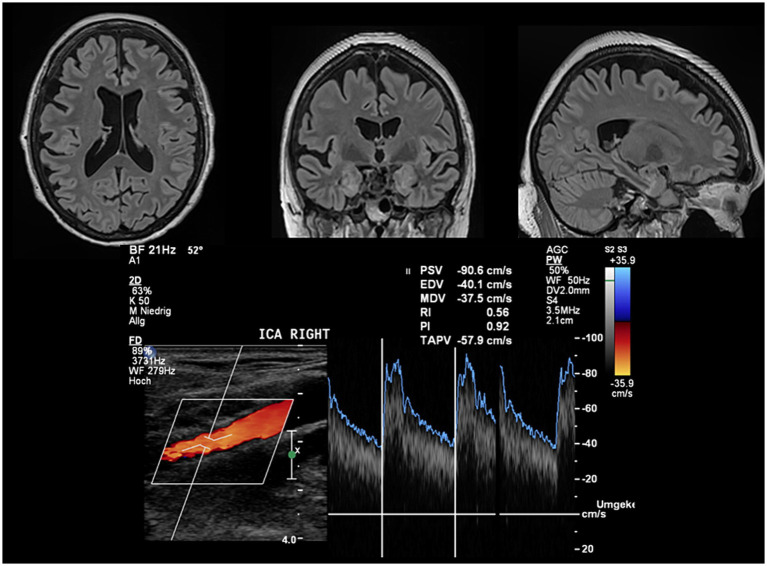
This prospective single-center study recruited patients aged ≥60 years scheduled for elective spine surgery at a German university hospital. Patients underwent pre-operative assessments including cognitive abilities (CERAD test battery), structural MRI, and cerebrovascular duplex sonography. POD screening was conducted three times daily for at least 3 days. The primary hypothesis, that the mean pulsatility index (PI) of both internal carotid arteries (ICA) predicts POD risk, was tested using logistic regression. Secondary analyses examined the association between POD risk and ICA flow (time-averaged peak velocities, TAPV) and correlations with cognitive profiles and MRI characteristics.
POD occurred in 22% of patients ( = 22/99) within three postoperative days. Patients with POD were significantly older (75.9 ± 5.4 vs. 70.0 ± 6.9 years, < 0.01) but did not differ by gender ( = 0.51). ICA PI significantly predicted POD risk (OR = 5.46 [95%CI: 1.81-16.49], = 0.003), which remained significant after adjustment for age and duration of surgery (OR = 6.38 [95% CI: 1.77-23.03], = 0.005). TAPV did not inform the POD risk ( = 0.68). ICA PI Pre-operative cognitive scores were significantly associated with ICA PI (mean CERAD score: = -0.32, < 0.001). ICA PI was also significantly associated with total white matter lesion volume ( = 0.19, = 0.012) and periventricular white matter lesion volume ( = 0.21, = 0.007).
This is the first study to demonstrate that cerebrovascular duplex sonography can assess the risk for POD in elderly spine surgery patients. Increased ICA PI may indicate subcortical impairment, larger white matter lesion load, and lower white matter volume, predisposing factors for POD. Pre-operative cerebrovascular duplex sonography of the ICA is widely available, easy-to-use, and efficient, offering a promising screening method for POD risk. Increased ICA PI could supplement established predictors like age to adjust surgical and peri-operative procedures to individual risk profiles.
脊柱手术的进展使得对老年患者进行安全干预成为可能,但围手术期神经认知障碍(pNCD),如术后谵妄(POD)和认知功能障碍(POCD),仍然是一个严重问题。术前认知障碍是pNCD的主要危险因素。在临床实践中进行全面的术前认知评估并不可行,因此需要有效的筛查方法。本研究调查术前脑血管双功超声检查是否可以评估皮质下(血管性)认知障碍和POD风险。
这项前瞻性单中心研究招募了德国一家大学医院计划进行择期脊柱手术的≥60岁患者。患者接受了术前评估,包括认知能力(CERAD测试组)、结构MRI和脑血管双功超声检查。每天对POD进行至少3天的三次筛查。使用逻辑回归检验主要假设,即双侧颈内动脉(ICA)的平均搏动指数(PI)预测POD风险。二次分析检查了POD风险与ICA血流(时间平均峰值速度,TAPV)之间的关联以及与认知特征和MRI特征的相关性。
22%的患者(n = 22/99)在术后三天内发生POD。发生POD的患者年龄显著更大(75.9±5.4岁对70.0±6.9岁,P < 0.01),但在性别上无差异(P = 0.51)。ICA PI显著预测POD风险(OR = 5.46 [95%CI:1.81 - 16.49],P = 让我重新为你翻译这段内容:
脊柱手术的进展使老年患者能得到安全干预,但围手术期神经认知障碍(pNCD),如术后谵妄(POD)和认知功能障碍(POCD),仍是严重问题。术前认知障碍是pNCD的主要危险因素。临床实践中全面的术前认知评估不可行,因此需要有效的筛查方法。本研究调查术前脑血管双功超声能否评估皮质下(血管性)认知障碍及POD风险。
这项前瞻性单中心研究纳入德国一家大学医院计划行择期脊柱手术、年龄≥60岁的患者。患者接受术前评估,包括认知能力(CERAD测试组)、结构磁共振成像(MRI)和脑血管双功超声检查。每天至少3次对POD进行筛查,持续至少3天。使用逻辑回归检验主要假设,即双侧颈内动脉(ICA)的平均搏动指数(PI)预测POD风险。二次分析检查POD风险与ICA血流(时间平均峰值速度,TAPV)的关联以及与认知特征和MRI特征的相关性。
22%的患者(n = 22/99)在术后3天内发生POD。发生POD的患者年龄显著更大(75.9±5.4岁对70.0±6.9岁,P < 0.01),但性别无差异(P = 0.51)。ICA PI显著预测POD风险(OR = 5.46 [95%CI:1.81 - 16.49],P = 0.003),在调整年龄和手术时长后仍显著(OR = 6.38 [95%CI:1.7