Abdelrahim A, Ali O, Kamali D, Reddy A, Harrison S, Boshnaq M, Abudeeb H, Ashoush F, Qulaghassi M, Eldesouky S, Mansour M, Rahman-Casans S F, Osman K
Health Education England Northeast, UK.
East Lancashire Hospitals NHS Foundation Trust, UK.
Ann R Coll Surg Engl. 2025 May;107(5):326-330. doi: 10.1308/rcsann.2024.0077. Epub 2024 Oct 9.
The aim of this study was to assess the yield of the endoscopic investigations performed following the resolution of acute diverticulitis.
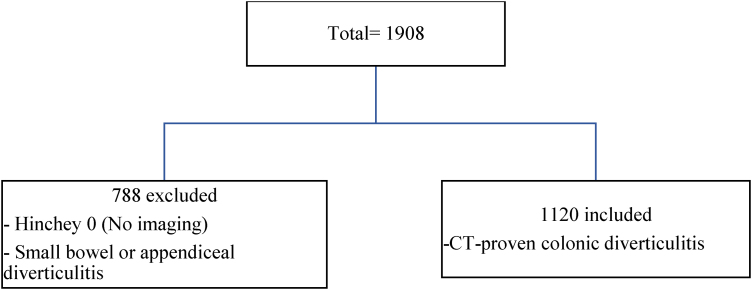
A retrospective multicentre study included patients with multislice computed tomography (MSCT)-proven diverticulitis, in four NHS hospitals, between January 2016 and April 2023. The primary outcome was the rate of colonic cancer in the diseased segment. Secondary outcomes included the rate of malignancy in the nondiseased colonic segments, the benign colonic polyp detection rate, the rate of malignancy in the resected surgical specimens in patients who underwent an emergency surgery on the index admission and the rate of complications in the investigated group.
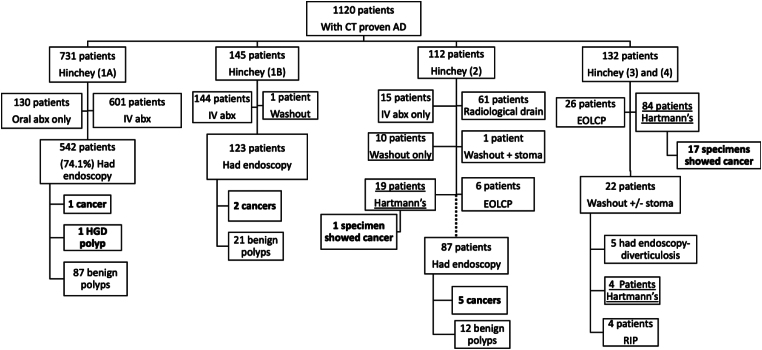
A total of 1,120 patients were included in the study, out of which 604 were females, with a median age of 61 years; 731 patients (65%) had uncomplicated diverticulitis (Hinchey 1A) while 389 (35%) had complicated diverticulitis (Hinchey 1B-4). Following the acute episode, 757 (74%) patients had subsequent endoscopic evaluation. The incidence of colorectal cancer (CRC) or advanced adenomas (AA) in patients with uncomplicated diverticulitis was 0.14%. In the complicated diverticulitis group, the incidence of CRC/AA in patients with Hinchey 1b and Hinchey 2 was 1.4% and 5.4%, respectively. Out of the 107 patients who underwent emergency colonic resection for suspected perforated diverticulitis, 18 (16.8%) had histological evidence of colonic malignancy.
Endoscopic investigations following uncomplicated diverticulitis have a low yield for sinister colonic pathology. Colonoscopy should be planned following complicated diverticulitis and in patients with uncomplicated diverticulitis with suspicious radiological finding on index imaging or in patients with ongoing clinical manifestations. In patients who undergo emergency surgery, oncological principles should be applied whenever possible.
本研究的目的是评估急性憩室炎缓解后进行的内镜检查的诊断价值。
一项回顾性多中心研究纳入了2016年1月至2023年4月期间在四家国民保健服务(NHS)医院中经多层螺旋计算机断层扫描(MSCT)证实患有憩室炎的患者。主要结局是病变节段的结肠癌发生率。次要结局包括非病变结肠段的恶性肿瘤发生率、良性结肠息肉检出率、因本次入院接受急诊手术的患者切除的手术标本中的恶性肿瘤发生率以及研究组的并发症发生率。
本研究共纳入1120例患者,其中604例为女性,中位年龄61岁;731例患者(65%)患有非复杂性憩室炎(欣奇1A),389例(35%)患有复杂性憩室炎(欣奇1B - 4)。急性发作后,757例(74%)患者随后接受了内镜评估。非复杂性憩室炎患者中结直肠癌(CRC)或高级别腺瘤(AA)的发生率为0.14%。在复杂性憩室炎组中,欣奇1b和欣奇2患者的CRC/AA发生率分别为1.4%和5.4%。在因疑似穿孔性憩室炎接受急诊结肠切除术的107例患者中,18例(16.8%)有结肠恶性肿瘤的组织学证据。
非复杂性憩室炎后的内镜检查对严重结肠病变的诊断价值较低。对于复杂性憩室炎患者以及非复杂性憩室炎但初始影像学检查有可疑发现或有持续临床表现的患者,应安排结肠镜检查。对于接受急诊手术的患者,应尽可能遵循肿瘤学原则。