Mendell Jerry R, Muntoni Francesco, McDonald Craig M, Mercuri Eugenio M, Ciafaloni Emma, Komaki Hirofumi, Leon-Astudillo Carmen, Nascimento Andrés, Proud Crystal, Schara-Schmidt Ulrike, Veerapandiyan Aravindhan, Zaidman Craig M, Guridi Maitea, Murphy Alexander P, Reid Carol, Wandel Christoph, Asher Damon R, Darton Eddie, Mason Stefanie, Potter Rachael A, Singh Teji, Zhang Wenfei, Fontoura Paulo, Elkins Jacob S, Rodino-Klapac Louise R
Center for Gene Therapy, Nationwide Children's Hospital, Columbus, OH, USA.
The Ohio State University, Columbus, OH, USA.
Nat Med. 2025 Jan;31(1):332-341. doi: 10.1038/s41591-024-03304-z. Epub 2024 Oct 9.
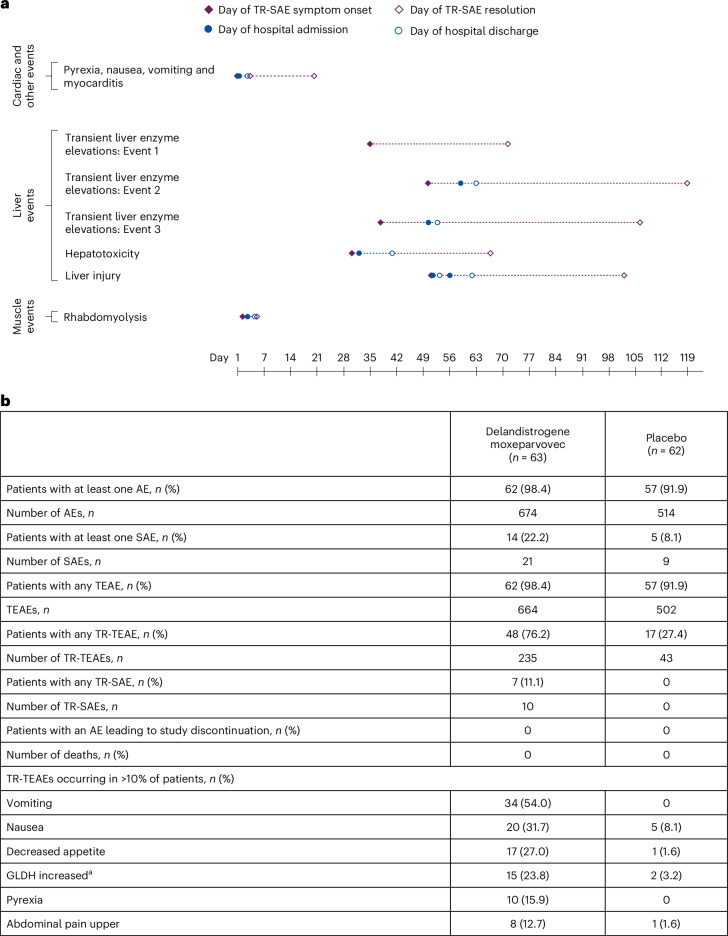
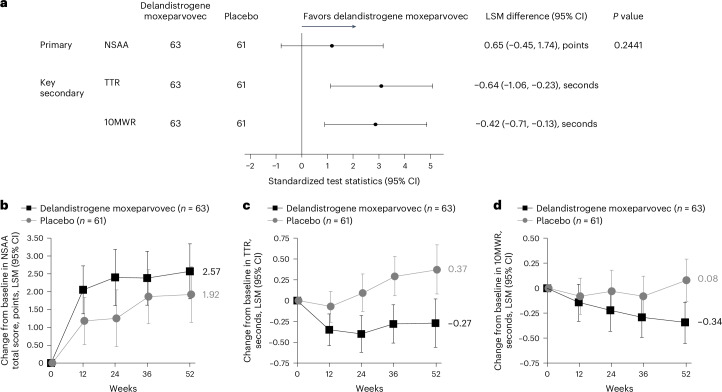
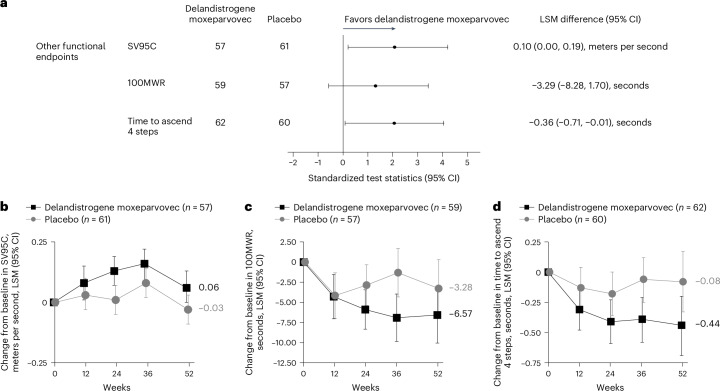
Duchenne muscular dystrophy (DMD) is a rare, X-linked neuromuscular disease caused by pathogenic variants in the DMD gene that result in the absence of functional dystrophin, beginning at birth and leading to progressive impaired motor function, loss of ambulation and life-threatening cardiorespiratory complications. Delandistrogene moxeparvovec, an adeno-associated rh74-viral vector-based gene therapy, addresses absent functional dystrophin in DMD. Here the phase 3 EMBARK study aimed to assess the efficacy and safety of delandistrogene moxeparvovec in patients with DMD. Ambulatory males with DMD, ≥4 years to <8 years of age, were randomized and stratified by age group and North Star Ambulatory Assessment (NSAA) score to single-administration intravenous delandistrogene moxeparvovec (1.33 × 10 vector genomes per kilogram; n = 63) or placebo (n = 62). At week 52, the primary endpoint, change from baseline in NSAA score, was not met (least squares mean 2.57 (delandistrogene moxeparvovec) versus 1.92 (placebo) points; between-group difference, 0.65; 95% confidence interval (CI), -0.45, 1.74; P = 0.2441). Secondary efficacy endpoints included mean micro-dystrophin expression at week 12: 34.29% (treated) versus 0.00% (placebo). Other secondary efficacy endpoints at week 52 (between-group differences (95% CI)) included: Time to Rise (-0.64 (-1.06, -0.23)), 10-meter Walk/Run (-0.42 (-0.71, -0.13)), stride velocity 95th centile (0.10 (0.00, 0.19)), 100-meter Walk/Run (-3.29 (-8.28, 1.70)), time to ascend 4 steps (-0.36 (-0.71, -0.01)), PROMIS Mobility and Upper Extremity (0.05 (-0.08, 0.19); -0.04 (-0.24, 0.17)) and number of NSAA skills gained/improved (0.19 (-0.67, 1.06)). In total, 674 adverse events were recorded with delandistrogene moxeparvovec and 514 with placebo. There were no deaths, discontinuations or clinically significant complement-mediated adverse events; 7 patients (11.1%) experienced 10 treatment-related serious adverse events. Delandistrogene moxeparvovec did not lead to a significant improvement in NSAA score at week 52. Some of the secondary endpoints numerically favored treatment, although no statistical significance can be claimed. Safety was manageable and consistent with previous delandistrogene moxeparvovec trials. ClinicalTrials.gov: NCT05096221.
杜氏肌营养不良症(DMD)是一种罕见的X连锁神经肌肉疾病,由DMD基因中的致病变异引起,导致功能性抗肌萎缩蛋白缺失,从出生时就开始出现,并导致进行性运动功能受损、行走能力丧失以及危及生命的心肺并发症。德蓝地昔单抗莫克帕罗韦(delandistrogene moxeparvovec)是一种基于腺相关rh74病毒载体的基因疗法,用于解决DMD中功能性抗肌萎缩蛋白缺失的问题。在此,3期EMBARK研究旨在评估德蓝地昔单抗莫克帕罗韦对DMD患者的疗效和安全性。年龄≥4岁至<8岁的DMD门诊男性患者按年龄组和北极星门诊评估(NSAA)评分进行随机分组和分层,分别接受单次静脉注射德蓝地昔单抗莫克帕罗韦(每千克1.33×10个载体基因组;n = 63)或安慰剂(n = 62)。在第52周时,未达到主要终点,即NSAA评分较基线的变化(最小二乘均值:德蓝地昔单抗莫克帕罗韦组为2.57分,安慰剂组为1.92分;组间差异为0.65;95%置信区间(CI)为-0.45,1.74;P = 0.2441)。次要疗效终点包括第12周时的平均微抗肌萎缩蛋白表达:治疗组为34.29%,安慰剂组为0.00%。第52周时的其他次要疗效终点(组间差异(95%CI))包括:起身时间(-0.64(-1.06,-0.23))、10米步行/跑步(-0.42(-0.71,-0.13))、第95百分位步幅速度(0.10(0.00,0.19))、100米步行/跑步(-3.29(-8.28,1.70))、上4级台阶时间(-0.36(-0.71,-0.01))、患者报告结果测量信息系统(PROMIS)活动能力和上肢功能(0.05(-0.08,0.19);-0.04(-0.24,0.17))以及获得/改善的NSAA技能数量(0.19(-0.67,1.06))。德蓝地昔单抗莫克帕罗韦组共记录了674起不良事件,安慰剂组记录了514起。没有死亡、停药或具有临床意义的补体介导的不良事件;7名患者(11.1%)发生了10起与治疗相关的严重不良事件。在第52周时,德蓝地昔单抗莫克帕罗韦并未使NSAA评分得到显著改善。一些次要终点在数值上有利于治疗,尽管无法宣称具有统计学意义。安全性可控,与之前的德蓝地昔单抗莫克帕罗韦试验一致。临床试验.gov标识符:NCT05096221。