Mouchantaf Mark, Parisi Marco, Secci Gregorio, Biegun Manon, Chelli Mikael, Schippers Philipp, Boileau Pascal
Institut de Chirurgie Réparatrice (ICR), Locomoteur & Sports, Nice, France.
Bone Jt Open. 2024 Oct 10;5(10):851-857. doi: 10.1302/2633-1462.510.BJO-2024-0097.R1.
Optimal glenoid positioning in reverse shoulder arthroplasty (RSA) is crucial to provide impingement-free range of motion (ROM). Lateralization and inclination correction are not yet systematically used. Using planning software, we simulated the most used glenoid implant positions. The primary goal was to determine the configuration that delivers the best theoretical impingement-free ROM.
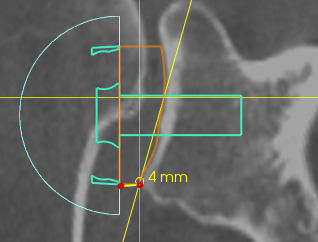
With the use of a 3D planning software (Blueprint) for RSA, 41 shoulders in 41 consecutive patients (17 males and 24 females; means age 73 years (SD 7)) undergoing RSA were planned. For the same anteroposterior positioning and retroversion of the glenoid implant, four different glenoid baseplate configurations were used on each shoulder to compare ROM: 1) no correction of the RSA angle and no lateralization (C-L-); 2) correction of the RSA angle with medialization by inferior reaming (C+M+); 3) correction of the RSA angle without lateralization by superior compensation (C+L-); and 4) correction of the RSA angle and additional lateralization (C+L+). The same humeral inlay implant and positioning were used on the humeral side for the four different glenoid configurations with a 3 mm symmetric 135° inclined polyethylene liner.
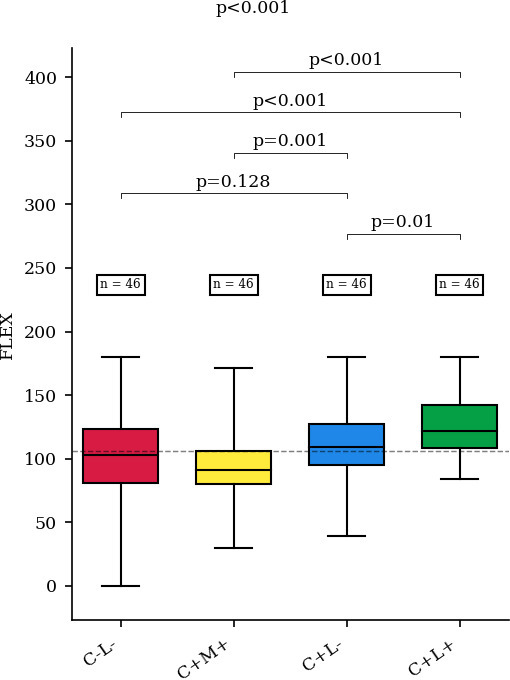
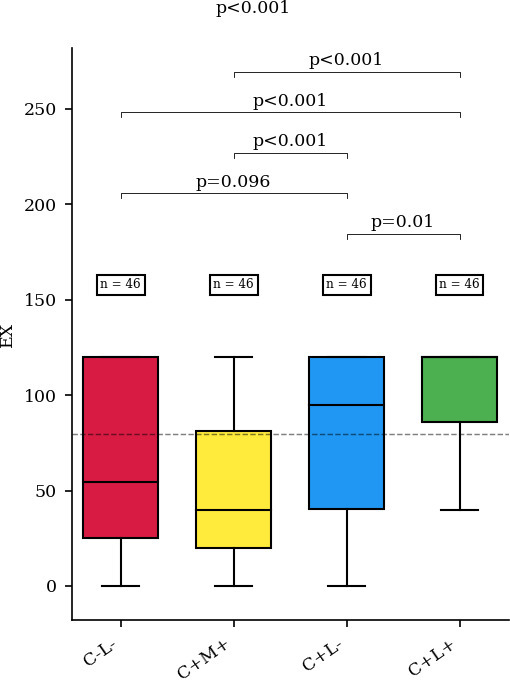
The configuration with lateralization and correction of the RSA angle (C+L+) led to better ROM in flexion, extension, adduction, and external rotation (p ≤ 0.001). Only internal rotation was not significantly different between groups (p = 0.388). The configuration where correction of the inclination was done by medialization (C+M+) led to the worst ROM in adduction, extension, abduction, flexion, and external rotation of the shoulder.
Our software study shows that, when using a 135° inlay reversed humeral implant, correcting glenoid inclination (RSA angle 0°) and lateralizing the glenoid component by using an angled bony or metallic augment of 8 to 10 mm provides optimal impingement-free ROM.
在反肩关节置换术(RSA)中,最佳的关节盂定位对于实现无撞击的活动范围(ROM)至关重要。目前尚未系统地采用关节盂的侧方移位和倾斜度矫正。我们使用规划软件模拟了最常用的关节盂植入物位置。主要目标是确定能提供最佳理论无撞击ROM的配置。
使用用于RSA的三维规划软件(Blueprint),对41例连续接受RSA的患者(17例男性和24例女性;平均年龄73岁(标准差7岁))的41个肩部进行规划。对于相同的关节盂植入物前后位定位和后倾角,每个肩部使用四种不同的关节盂基板配置来比较ROM:1)不矫正RSA角且无侧方移位(C-L-);2)通过下方扩孔进行RSA角矫正并向内侧移位(C+M+);3)通过上方补偿矫正RSA角但无侧方移位(C+L-);4)矫正RSA角并额外进行侧方移位(C+L+)。对于四种不同的关节盂配置,在肱骨侧使用相同的肱骨嵌体植入物和定位,采用3毫米对称135°倾斜的聚乙烯衬垫。
RSA角侧方移位并矫正(C+L+)的配置在屈曲、伸展、内收和外旋方面导致更好的ROM(p≤0.001)。仅内旋在各组之间无显著差异(p = 0.388)。通过向内侧移位进行倾斜度矫正(C+M+)的配置在肩部内收、伸展、外展、屈曲和外旋方面导致最差的ROM。
我们的软件研究表明,当使用135°嵌体式反向肱骨植入物时,通过使用8至10毫米的成角骨质或金属增强物矫正关节盂倾斜度(RSA角0°)并使关节盂组件侧方移位可提供最佳的无撞击ROM。