Liu Alice J, Dennis Adelaide S M, Fariha Zarin, Pai Mangalore Rekha, Macesic Nenad
Department of Infectious Diseases, The Alfred Hospital and School of Translational Medicine, Monash University, Melbourne, Australia.
Centre to Impact AMR, Monash University, Clayton, Australia.
JAC Antimicrob Resist. 2024 Oct 9;6(5):dlae152. doi: 10.1093/jacamr/dlae152. eCollection 2024 Oct.
Bloodstream infections (BSIs) cause significant morbidity and mortality in solid organ transplant (SOT) recipients. There are few data regarding the contribution of MDR organisms (MDROs) to these infections. We evaluated the resistance percentage of MDRO BSIs in SOT recipients and the associated mortality.
A systematic review of MEDLINE and Embase databases up to January 2024, for studies of adult SOT recipients that quantified MDRO BSI resistance percentage and/or associated crude mortality. MDROs studied were carbapenem-resistant Enterobacterales (CRE), (CRAB) and (CRPA), third-generation cephalosporin-resistant Enterobacterales (3GCR-E), MRSA and VRE. Resistance percentage and mortality outcomes were reported as median (IQR) and crude mortality (%), respectively.
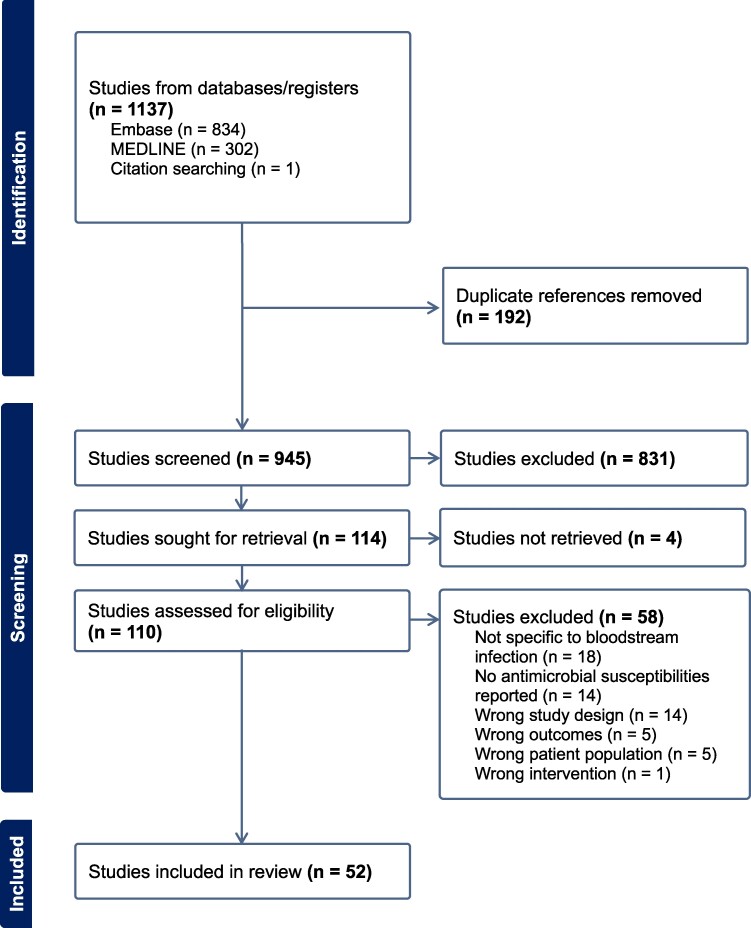
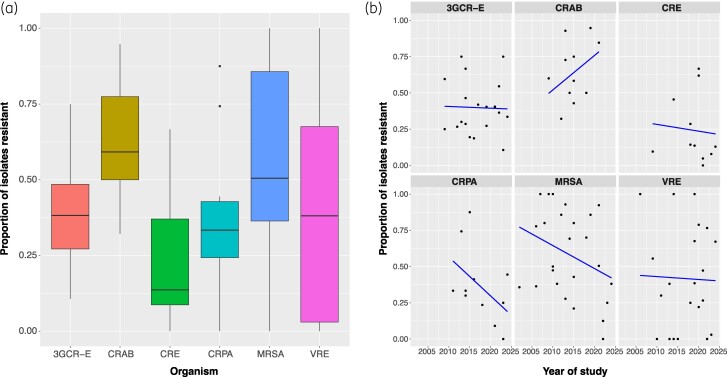
Of 945 studies identified, 52 were included. Most were retrospective (41/52) and/or single centre (37/52), and liver transplantation was the most frequently studied SOT type (22/52). High resistance percentages of BSIs were noted, ranging from 13.6% CRE for Enterobacterales to 59.2% CRAB for . Resistance percentage trends decreased over time, but these changes were not statistically significant. Asia had the highest resistance percentages for MRSA [86.2% (IQR 77.3%-94.6%)], 3GCR-E [59.5% (IQR 40.5%-66.7%)] and CRE [35.7% (IQR 8.3%-63.1%)]. North America had the highest VRE resistance percentages [77.7% (IQR 54.6%-94.7%)]. Crude mortality was 15.4%-82.4% and was consistently higher than for non-MDRO BSIs.
MDRO BSI resistance percentages were high for all pathogens studied (IQR 24.6%-69.4%) but there was geographical and temporal heterogeneity. MDRO BSIs were associated with high mortality in SOT recipients. Microbiological and clinical data in this vulnerable population were incomplete, highlighting the need for robust international multicentre studies.
血流感染(BSIs)在实体器官移植(SOT)受者中会导致显著的发病率和死亡率。关于多重耐药菌(MDROs)对这些感染的影响的数据很少。我们评估了SOT受者中MDRO血流感染的耐药百分比及相关死亡率。
对截至2024年1月的MEDLINE和Embase数据库进行系统综述,纳入量化MDRO血流感染耐药百分比和/或相关粗死亡率的成年SOT受者研究。所研究的MDROs包括耐碳青霉烯类肠杆菌科细菌(CRE)、耐碳青霉烯类鲍曼不动杆菌(CRAB)和耐碳青霉烯类铜绿假单胞菌(CRPA)、耐第三代头孢菌素肠杆菌科细菌(3GCR-E)、耐甲氧西林金黄色葡萄球菌(MRSA)和耐万古霉素肠球菌(VRE)。耐药百分比和死亡率结果分别报告为中位数(四分位间距)和粗死亡率(%)。
在945项检索到的研究中,纳入了52项。大多数研究为回顾性研究(41/52)和/或单中心研究(37/52),肝移植是研究最频繁的SOT类型(22/52)。注意到血流感染的耐药百分比很高,从肠杆菌科细菌的CRE为13.6%到鲍曼不动杆菌的CRAB为59.2%不等。耐药百分比趋势随时间下降,但这些变化无统计学意义。亚洲的MRSA [86.2%(四分位间距77.3%-94.6%)]、3GCR-E [59.5%(四分位间距40.5%-66.7%)]和CRE [35.7%(四分位间距8.3%-63.1%)]耐药百分比最高。北美的VRE耐药百分比最高[77.7%(四分位间距54.6%-94.7%)]。粗死亡率为15.4%-82.4%,且始终高于非MDRO血流感染。
所有研究病原体的MDRO血流感染耐药百分比都很高(四分位间距24.6%-69.4%),但存在地理和时间异质性。MDRO血流感染与SOT受者的高死亡率相关。这一脆弱人群的微生物学和临床数据不完整,凸显了开展有力的国际多中心研究的必要性。