Terry Merryl, Nguyen Minh P, Tang Vivian, Guney Ekin, Bharani Krishna L, Dahiya Sonika, Choutka Ondrej, Borys Ewa, Reis Gerald, Blevins Lewis, Aghi Manish K, Kunwar Sandeep, DeGroot John, Raleigh David R, Pekmezci Melike, Bollen Andrew W, Cha Soonmee, Joseph Nancy M, Perry Arie
Department of Pathology, Division of Neuropathology, University of California San Francisco, San Francisco, CA, USA.
Department of Pathology, Stanford University, Palo Alto, CA, USA.
Endocr Pathol. 2024 Dec;35(4):338-348. doi: 10.1007/s12022-024-09829-w. Epub 2024 Oct 10.
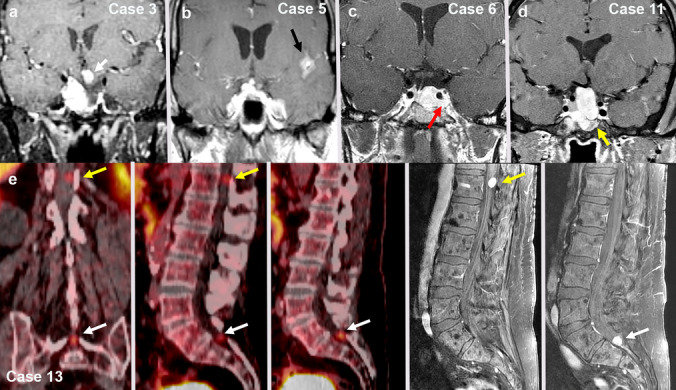
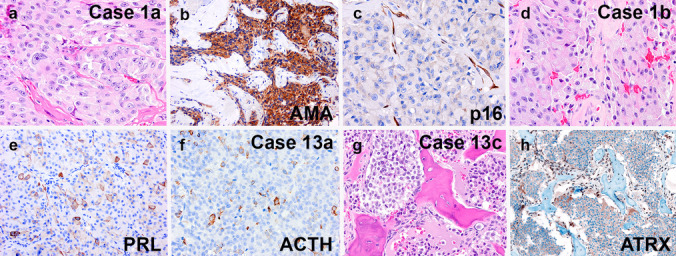
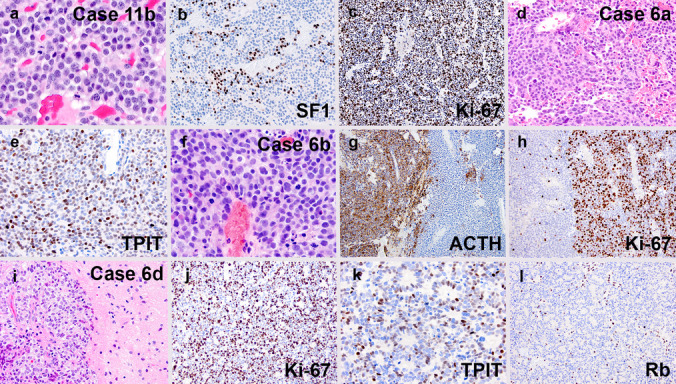
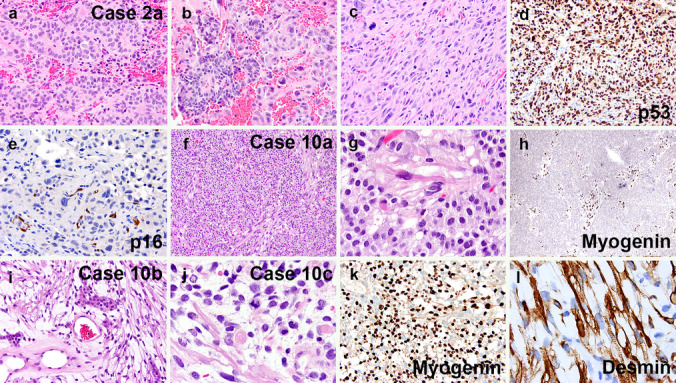
Pituitary neuroendocrine tumors (PitNET) that metastasize comprise ~ 0.2% of adenohypophyseal tumors are aggressive and are challenging to treat. However, many non-metastatic tumors are also aggressive. Herein, we review 21 specimens from 13 patients at UCSF with metastatic PitNETs (CSF or systemic, N = 7 patients), high-grade pituitary neuroendocrine neoplasms (HG-PitNEN, N = 4 patients), and/or PitNETs with sarcomatous transformation (PitNET-ST, N = 5 patients). We subtyped cases using the World Health Organization (WHO) and International Agency for Research on Cancer (IARC) criteria for neuroendocrine neoplasms (NENs). Lineage subtypes included acidophil stem cell, null cell, thyrotroph, corticotroph, lactotroph, and gonadotroph tumors. The median Ki-67 labeling index was 25% (range 5-70%). Lack of p16 was seen in 3 cases, with overexpression in 2. Strong diffuse p53 immunopositivity was present in 3 specimens from 2 patients. Loss of Rb expression was seen in 2 cases, with ATRX loss in one. Molecular analysis in 4 tumors variably revealed TERT alterations, homozygous CDKN2A deletion, aneuploidy, and mutations in PTEN, TP53, PDGFRB, and/or PIK3CA. Eight patients (62%) died of disease, 4 were alive at the last follow-up, and 1 was lost to the follow-up. All primary tumors had worrisome features, including aggressive lineage subtype, high mitotic count, and/or high Ki-67 indices. Additional evidence of high-grade progression included immunohistochemical loss of neuroendocrine, transcription factor, and/or hormone markers. We conclude that metastatic PitNET is not the only high-grade form of pituitary NEN. If further confirmed, these histopathologic and/or molecular features could provide advanced warning of biological aggressiveness and be applied towards a future grading scheme.
发生转移的垂体神经内分泌肿瘤(PitNET)占腺垂体肿瘤的0.2%左右,具有侵袭性,治疗颇具挑战。然而,许多非转移性肿瘤也具有侵袭性。在此,我们回顾了来自加州大学旧金山分校(UCSF)的13例患者的21份标本,这些患者患有转移性PitNET(脑脊液或全身转移,7例患者)、高级别垂体神经内分泌肿瘤(HG-PitNEN,4例患者)和/或伴有肉瘤样转化的PitNET(PitNET-ST,5例患者)。我们根据世界卫生组织(WHO)和国际癌症研究机构(IARC)的神经内分泌肿瘤(NEN)标准对病例进行亚型分类。谱系亚型包括嗜酸干细胞、无功能细胞、促甲状腺激素细胞、促肾上腺皮质激素细胞、催乳素细胞和促性腺激素细胞肿瘤。Ki-67标记指数的中位数为25%(范围5%-70%)。3例可见p16缺失,2例过表达。2例患者的3份标本中存在强烈弥漫性p53免疫阳性。2例可见Rb表达缺失,1例存在ATRX缺失。4例肿瘤的分子分析不同程度地显示了TERT改变、纯合性CDKN2A缺失、非整倍体以及PTEN、TP53、PDGFRB和/或PIK3CA突变。8例患者(62%)死于疾病,4例在最后一次随访时存活,1例失访。所有原发性肿瘤均具有令人担忧的特征,包括侵袭性谱系亚型、高有丝分裂计数和/或高Ki-67指数。高级别进展的其他证据包括神经内分泌、转录因子和/或激素标志物的免疫组化缺失。我们得出结论,转移性PitNET并非垂体NEN的唯一高级别形式。如果得到进一步证实,这些组织病理学和/或分子特征可为生物学侵袭性提供早期预警,并应用于未来的分级方案。