PGIMER, Chandigarh, India.
Department of Cardiology, CH(AF), Bengaluru, India.
Indian Heart J. 2024 Sep-Oct;76(5):327-332. doi: 10.1016/j.ihj.2024.10.001. Epub 2024 Oct 10.
Difficult coronary sinus (CS) anatomy may lead to difficulty in optimal left ventricular (LV) lead placement and lead displacements leading to nonresponse to cardiac resynchronization therapy (CRT).
In this retrospective study, we studied the CRT parameters of devices implanted by single operator during the time period from January 2014 till December 2021, where different off-label techniques were used to place/stabilize LV lead. The technique used to stabilize LV lead, CRT parameters at baseline and follow up were noted for each patient.
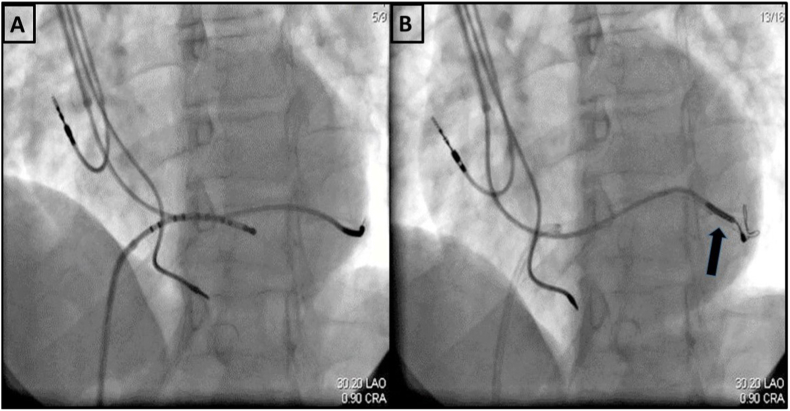
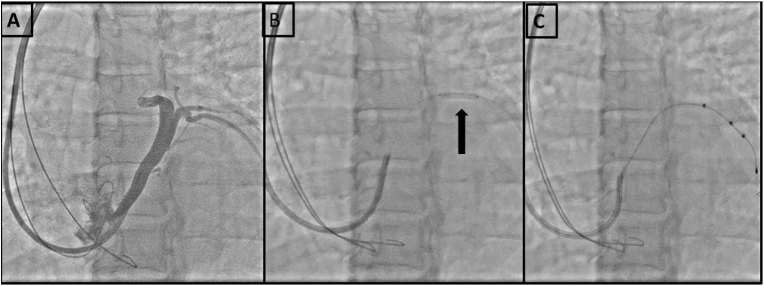
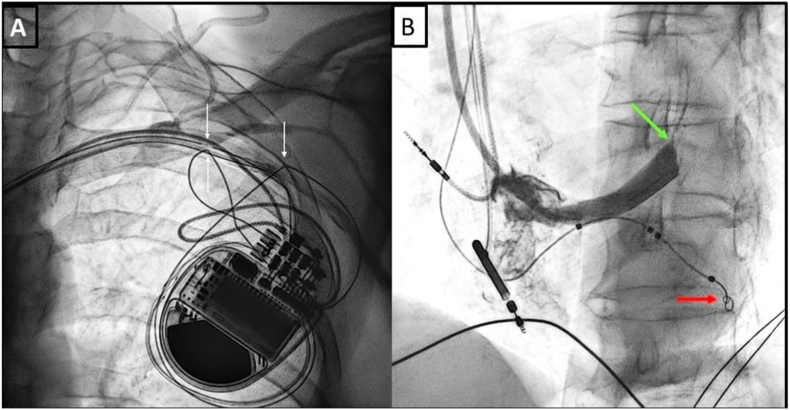
Out of 133 CRTs implanted during the study period, 23 patients (17.29 %) required off-label techniques. Stylet and guidewire retaining techniques were used in 11/23 (47.82 %) and 7/23 (30.43 %) patients respectively. In two patients, LV lead was jailed using coronary stent to prevent displacement. Two patients had CS stenosis and required balloon dilation while one patient had tortuous posterolateral vein which was straightened using a coronary stent. There was technical failure of 6/23 LV leads (26.08 %) with loss of capture, at a median follow up of 44 months (Range: 06-114 months). Out of these 6 patients, stylet and guidewire retaining techniques were used in 4 and 2 patients respectively.
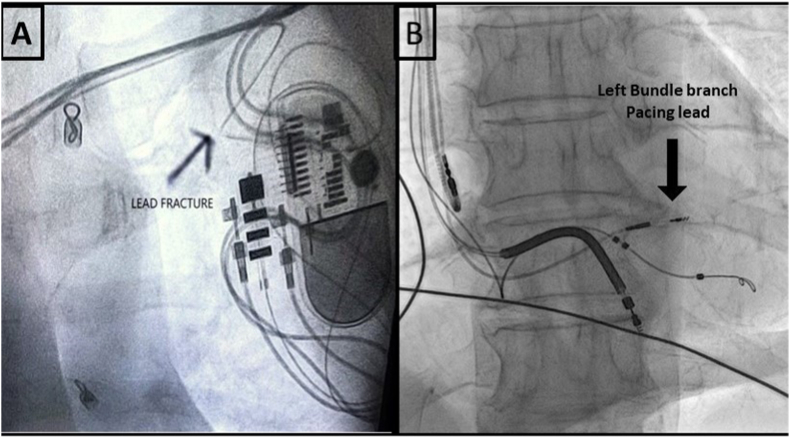
Despite having acceptable parameters at implantation, these techniques particularly stylet and guidewire retention, may lead to non-capture of LV lead on long term follow ups. Better LV leads like active fixation leads and conduction system pacing (His Bundle/left bundle branch pacing) should be preferred in difficult CS anatomy.
复杂的冠状窦(CS)解剖结构可能导致左心室(LV)导联的最佳放置困难,并导致导联移位,从而导致心脏再同步治疗(CRT)无反应。
在这项回顾性研究中,我们研究了 2014 年 1 月至 2021 年 12 月期间由单一操作者植入的 CRT 参数,在此期间使用了不同的标签外技术来放置/稳定 LV 导联。记录了每位患者使用的稳定 LV 导联的技术、基线和随访时的 CRT 参数。
在研究期间植入的 133 例 CRT 中,有 23 例(17.29%)需要使用标签外技术。在 23 例患者中,11 例(47.82%)和 7 例(30.43%)分别使用了钢丝和导丝保留技术。在两名患者中,LV 导联被冠状动脉支架固定以防止移位。两名患者 CS 狭窄,需要球囊扩张,一名患者后外侧静脉迂曲,使用冠状动脉支架拉直。23 例 LV 导联中有 6 例(26.08%)出现技术失败,失夺获,中位随访时间为 44 个月(范围:06-114 个月)。在这 6 名患者中,钢丝和导丝保留技术分别用于 4 名和 2 名患者。
尽管植入时参数可接受,但这些技术,特别是钢丝和导丝保留,可能会导致 LV 导联在长期随访中失夺获。在复杂 CS 解剖结构中,应优先使用更好的 LV 导联,如主动固定导联和传导系统起搏(希氏束/左束支起搏)。