ICU and Perioperative Medicine Hazm Mebaireek General Hospital HMC, Industrial Area Ar- Rayyan Doha, Doha, Qatar.
Department of Anesthesiology and Reanimation, University of Health Sciences, Istanbul, Turkey.
BMC Anesthesiol. 2024 Oct 11;24(1):367. doi: 10.1186/s12871-024-02755-8.
Pulse oximetry is a standart of anesthesia for perioperative monitoring. Due to the principles of Hb oxygen dissociation curve, peripheral oxygen saturation has an approximate sensitivity and specificity of 90% for the detection of hypoxemia.
The primary outcome of the study was to evaluate ORi as an early parameter to determine hypoxia in morbidly obese patients. The secondary outcome was to compare the effectiveness of ORi with SpO in non-obese patients.
Prospective, observational study.
Department of elective operating room at tertiary hospital.
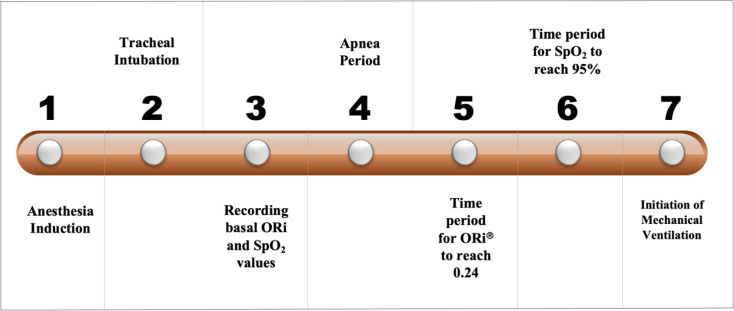
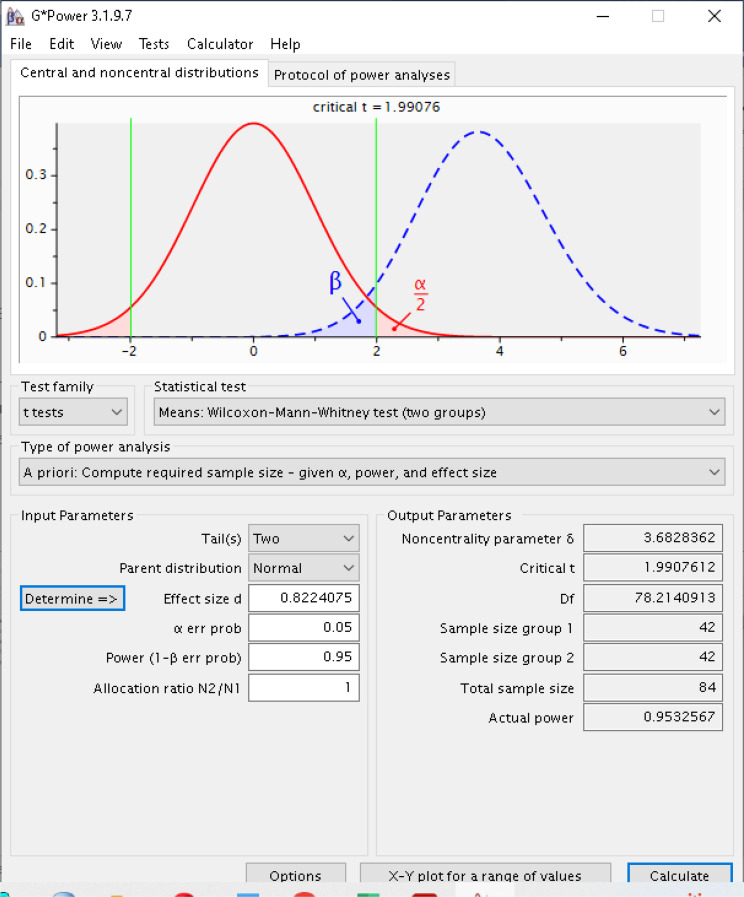
Observational study included written informed consent from 51 patients with 19 < BMI < 25 kg/m and 51 patients with BMI > 40 kg/m undergoing an elective surgery requiring tracheal intubation. In addition to standard monitors, an ORi sensor was placed and baseline values were recorded. The patients were preoxygenated until end tidal expiratory oxygen concentration is reached to 90%. After anesthesia induction and tracheal intubation, the breathing circuit was not connected tracheal tube until the SpO decreased to 95%. Shapiro-Wilk, Pearson Chi-square, t-test, and Mann Whitney U test were used for the study.
Times of tolerable apnea, ORi and SpO values at the end of preoxygenation, beginning of intubation, beginning of the ORi alarm, when SpO reached 95%, and when ORi reaches a plateau.
102 patients.
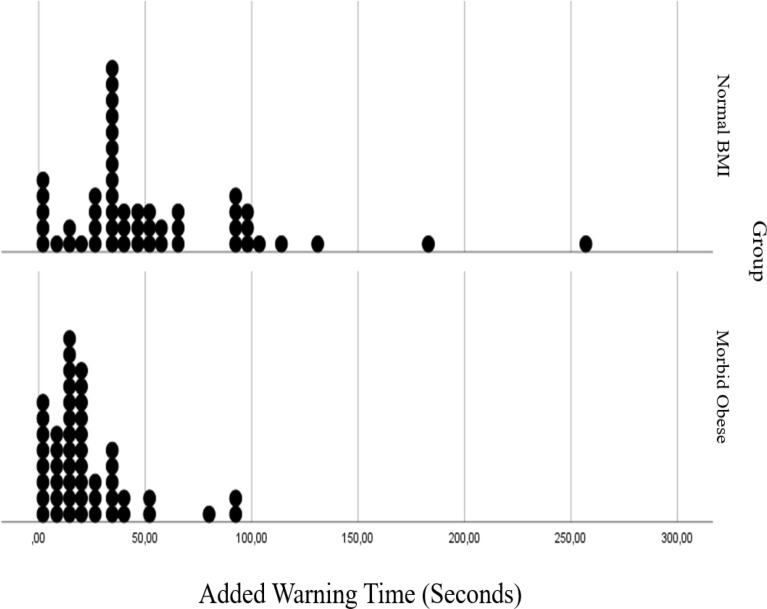
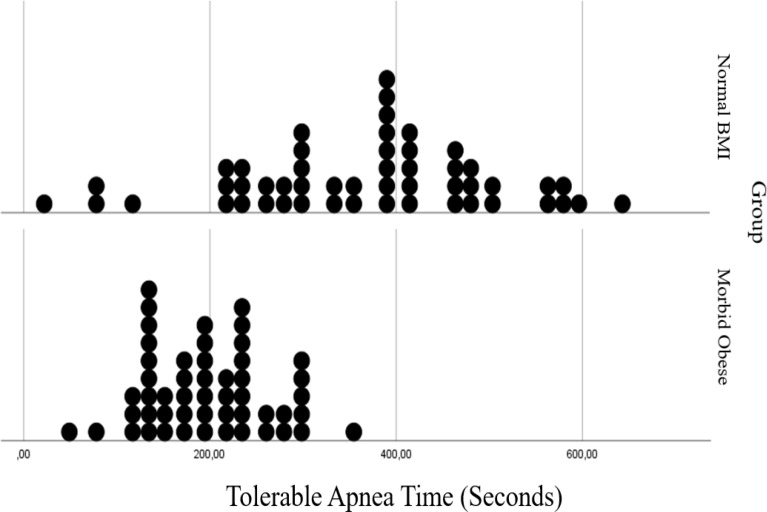
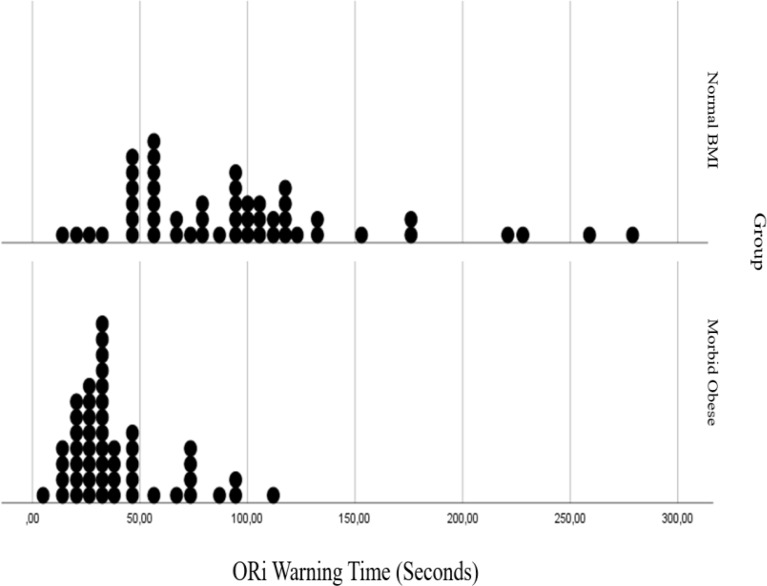
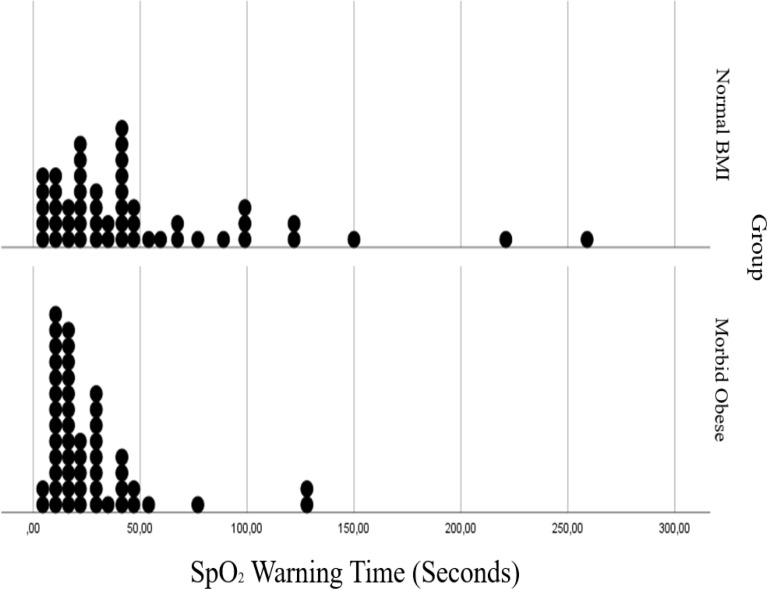
The alert period: time to reach ORi from 0.24 to a value of 95% SpO was observed as 32 s in morbidly obese patients and 94 s in patients with a normal body mass index. The SpO alert period was determined as time difference between 97% and 95% SpO. The data were recorded as 15 s and 36 s, respectively. It was observed that tolerable apnea, ORi, SpO and added alert times were longer in patients with normal BMI compared to morbidly obese patients.
As a result, ORi can provide an early warning to prevent unexpected hypoxia before saturation begins to decrease in morbidly obese patients.
Inability to perform arterial blood gas sampling in the time periods when we looked at the parameters to determine the relationship between ORi and PaO.
NCT05480748 registered 2022-07-29.
脉搏血氧饱和度监测是围手术期麻醉的标准。由于血红蛋白氧离解曲线的原理,外周氧饱和度对低氧血症的检测具有近似 90%的灵敏度和特异性。
本研究的主要结果是评估 ORi 作为一种早期参数来确定病态肥胖患者的缺氧情况。次要结果是比较 ORi 与非肥胖患者 SpO 的有效性。
前瞻性观察性研究。
三级医院择期手术室。
观察性研究包括 51 名 BMI 为 19< BMI <25 kg/m 和 51 名 BMI > 40 kg/m 的择期手术需要气管插管的肥胖患者的书面知情同意书。除了标准监测仪外,还放置了 ORi 传感器并记录了基线值。患者在达到呼气末呼出氧浓度 90%之前进行预充氧。麻醉诱导和气管插管后,在 SpO 下降到 95%之前,不连接气管导管。研究采用 Shapiro-Wilk、Pearson Chi-square、t 检验和 Mann Whitney U 检验。
可耐受的呼吸暂停时间、预充氧结束时、插管开始时、ORi 报警开始时、SpO 达到 95%时和 ORi 达到平台时的 ORi 和 SpO 值。
102 例。
报警期:ORi 从 0.24 增加到 95% SpO 的时间观察到肥胖患者为 32s,正常体重指数患者为 94s。SpO 报警期定义为 97%和 95% SpO 之间的时间差。数据分别记录为 15s 和 36s。与病态肥胖患者相比,正常体重指数患者的可耐受呼吸暂停时间、ORi、SpO 和附加报警时间更长。
结果表明,ORi 可以在肥胖患者饱和度开始下降之前,为防止意外缺氧提供早期预警。
在观察参数以确定 ORi 与 PaO 之间的关系时,无法在时间段内进行动脉血气采样。
NCT05480748 于 2022 年 7 月 29 日注册。