Heegaard Martin, Ingadottir Kristin, Ragborg Lærke, Dahl Benny, Hansen Lars Valentin, Ohrt-Nissen Søren, Gehrchen Martin
Spine Unit, Department of Orthopedic Surgery, Rigshospitalet, Copenhagen University Hospital, Copenhagen, Denmark.
Global Spine J. 2025 May;15(4):2218-2225. doi: 10.1177/21925682241291519. Epub 2024 Oct 13.
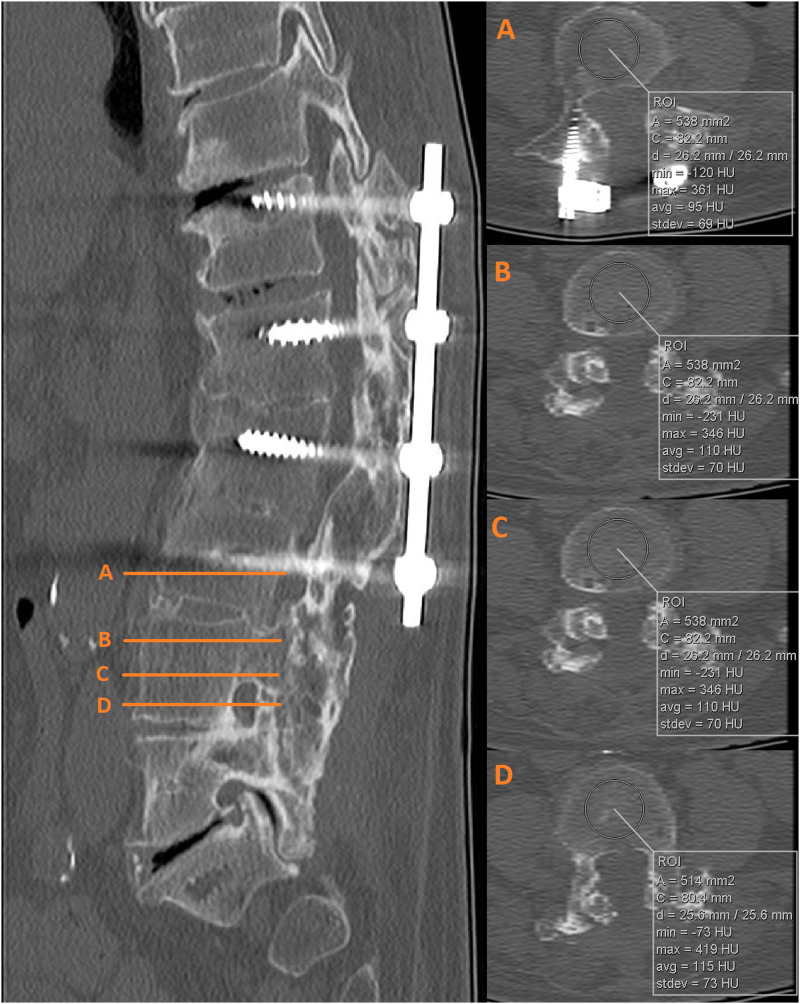
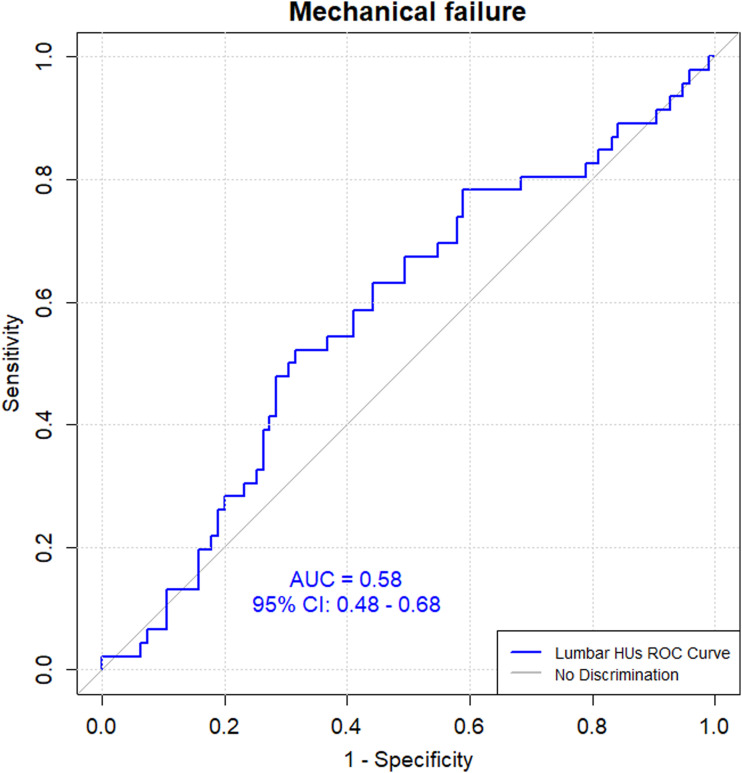
Study designRetrospective Cohort Study.ObjectivesLow bone mineral density (BMD) is a known risk factor for revision surgery in patients with adult spinal deformity (ASD). Hounsfield units (HUs) on CT scans have been suggested as a proxy for assessing BMD. This study aimed to determine HUs in the lumbar region and their association with mechanical failure in patients undergoing ASD surgery.MethodsWe included ASD patients undergoing surgery from 2010-2020 with minimum 2-year follow-up. We excluded patients without preoperative CT scans, or a CT scan more than 1 year before surgery. Mechanical failure was defined as proximal junctional failure, pseudarthrosis, or implant failure requiring revision surgery. On preoperative CT scans, HUs were measured on 3 axial slices on each vertebra from L1-L5 and, if available, at UIV and UIV + 1.ResultsWe included 170 patients, mean age 63 (±12) years, with 108 (64%) females, and 13 [IQR 10-16] instrumented levels. Mechanical failure occurred in 27% (n = 46) of patients at 2-year follow-up. Mean lumbar HUs were 146 (±51) in the mechanical failure group and 135 (±52) in those without revision ( = .232). Area under the curve was 0.58 (95% CI: 0.48-0.68), corresponding to no to low discriminatory power in predicting mechanical failure using lumbar HUs. Univariate logistic regression revealed no significant difference between mechanical failure and lumbar HUs (OR = 1.00, 95% CI: 1.00-1.01, = .239).ConclusionsWe found no association between mechanical failure and HUs on preoperative CT scans in ASD patients. Thus, we cannot recommend using HUs to predict mechanical failure in these patients.
研究设计
回顾性队列研究。
目的
低骨密度(BMD)是成人脊柱畸形(ASD)患者翻修手术的已知风险因素。CT扫描中的亨氏单位(HUs)已被建议作为评估骨密度的替代指标。本研究旨在确定ASD手术患者腰椎区域的亨氏单位及其与机械性失败的关联。
方法
我们纳入了2010年至2020年接受手术且至少随访2年的ASD患者。我们排除了没有术前CT扫描或手术前1年以上CT扫描的患者。机械性失败定义为近端交界性失败、假关节形成或需要翻修手术的植入物失败。在术前CT扫描上,从L1-L5在每个椎体的3个轴位切片上测量亨氏单位,如有可能,在UIV和UIV + 1处测量。
结果
我们纳入了170例患者,平均年龄63(±12)岁,其中108例(64%)为女性,平均固定节段数为13[四分位间距10-16]。在2年随访时,27%(n = 46)的患者发生了机械性失败。机械性失败组的平均腰椎亨氏单位为146(±51),未进行翻修的患者为135(±52)(P = 0.232)。曲线下面积为0.58(95%CI:0.48-0.68),这表明使用腰椎亨氏单位预测机械性失败的鉴别能力为无至低。单因素逻辑回归显示机械性失败与腰椎亨氏单位之间无显著差异(OR = 1.00,95%CI:1.00-1.01,P = 0.239)。
结论
我们发现ASD患者术前CT扫描上的机械性失败与亨氏单位之间无关联。因此,我们不建议使用亨氏单位来预测这些患者的机械性失败。