Lydon Emily, Osborne Christina M, Wagner Brandie D, Ambroggio Lilliam, Kirk Harris J, Reeder Ron, Carpenter Todd C, Maddux Aline B, Leroue Matthew K, Yehya Nadir, DeRisi Joseph L, Hall Mark W, Zuppa Athena F, Carcillo Joseph, Meert Kathleen, Sapru Anil, Pollack Murray M, McQuillen Patrick, Notterman Daniel A, Langelier Charles R, Mourani Peter M
Department of Medicine, University of California San Francisco, San Francisco, CA.
Department of Anesthesiology and Critical Care Medicine, Children's Hospital of Philadelphia, Philadelphia, PA.
bioRxiv. 2024 Oct 10:2024.10.08.617294. doi: 10.1101/2024.10.08.617294.
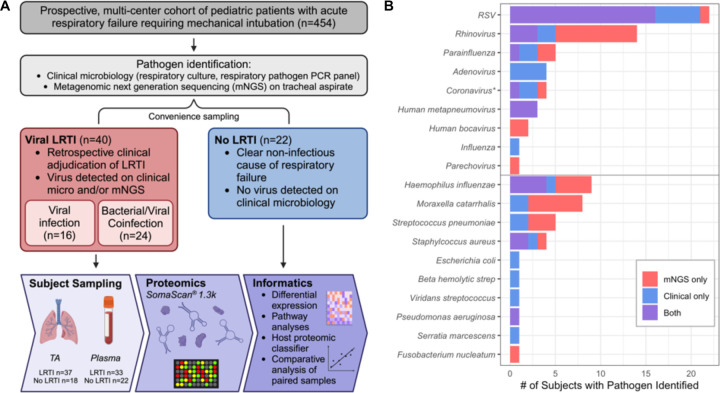
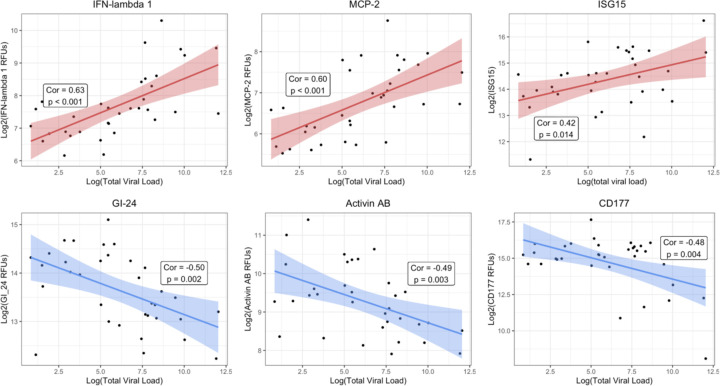
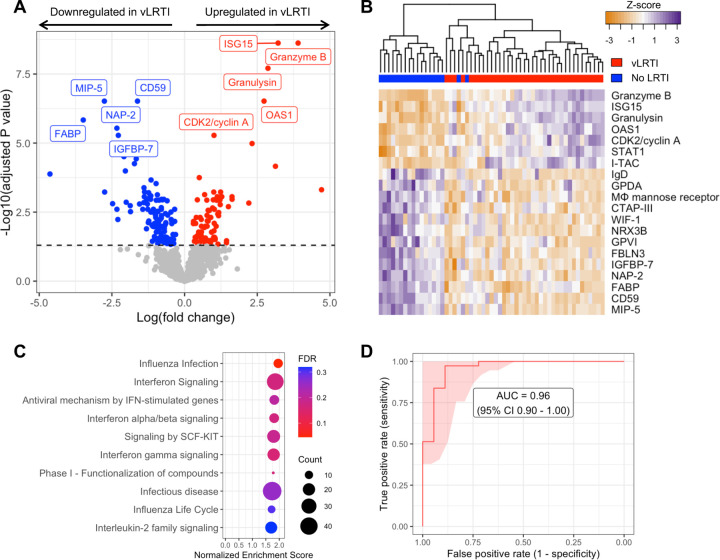
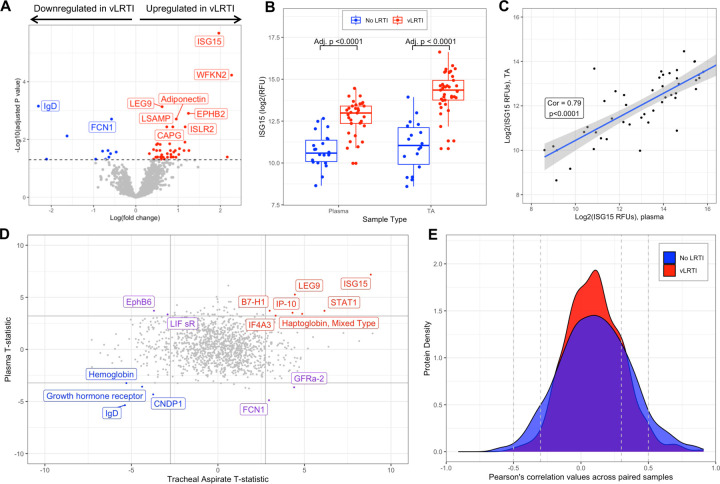
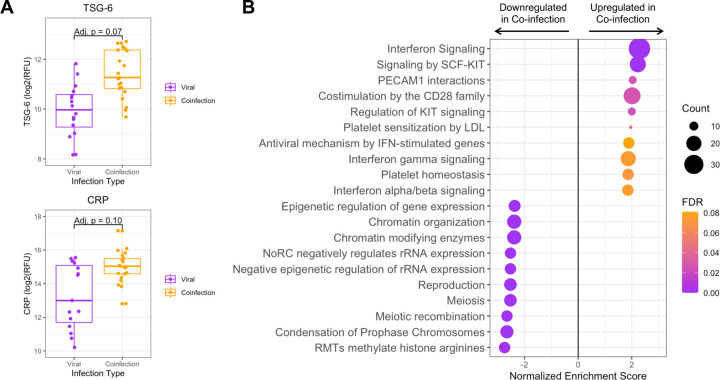
Viral lower respiratory tract infection (vLRTI) is a leading cause of hospitalization and death in children worldwide. Despite this, no studies have employed proteomics to characterize host immune responses to severe pediatric vLRTI in both the lower airway and systemic circulation. To address this gap, gain insights into vLRTI pathophysiology, and test a novel diagnostic approach, we assayed 1,305 proteins in tracheal aspirate (TA) and plasma from 62 critically ill children using SomaScan. We performed differential expression (DE) and pathway analyses comparing vLRTI (n=40) to controls with non-infectious acute respiratory failure (n=22), developed a diagnostic classifier using LASSO regression, and analyzed matched TA and plasma samples. We further investigated the impact of viral load and bacterial coinfection on the proteome. The TA signature of vLRTI was characterized by 200 DE proteins (P<0.05) with upregulation of interferons and T cell responses and downregulation of inflammation-modulating proteins including FABP and MIP-5. A nine-protein TA classifier achieved an AUC of 0.96 (95% CI 0.90-1.00) for identifying vLRTI. In plasma, the host response to vLRTI was more muted with 56 DE proteins. Correlation between TA and plasma was limited, although ISG15 was elevated in both compartments. In bacterial coinfection, we observed increases in the TNF-stimulated protein TSG-6, as well as CRP, and interferon-related proteins. Viral load correlated positively with interferon signaling and negatively with neutrophil-activation pathways. Taken together, our study provides fresh insight into the lower airway and systemic proteome of severe pediatric vLRTI, and identifies novel protein biomarkers with diagnostic potential.
病毒性下呼吸道感染(vLRTI)是全球儿童住院和死亡的主要原因。尽管如此,尚无研究采用蛋白质组学来表征下呼吸道和全身循环中宿主对严重儿童vLRTI的免疫反应。为了填补这一空白,深入了解vLRTI的病理生理学,并测试一种新的诊断方法,我们使用SomaScan检测了62名重症儿童气管吸出物(TA)和血浆中的1305种蛋白质。我们进行了差异表达(DE)和通路分析,将vLRTI组(n = 40)与非感染性急性呼吸衰竭对照组(n = 22)进行比较,使用套索回归开发了一种诊断分类器,并分析了匹配的TA和血浆样本。我们进一步研究了病毒载量和细菌合并感染对蛋白质组的影响。vLRTI的TA特征由200种差异表达蛋白(P<0.05)表征,其中干扰素和T细胞反应上调,包括FABP和MIP-5在内的炎症调节蛋白下调。一种九蛋白TA分类器在识别vLRTI方面的曲线下面积(AUC)为0.96(95%CI 0.90 - 1.00)。在血浆中,宿主对vLRTI的反应较为微弱,有56种差异表达蛋白。尽管ISG15在两个部位均升高,但TA与血浆之间的相关性有限。在细菌合并感染中,我们观察到TNF刺激蛋白TSG-6以及CRP和干扰素相关蛋白增加。病毒载量与干扰素信号呈正相关,与中性粒细胞激活途径呈负相关。综上所述,我们的研究为严重儿童vLRTI的下呼吸道和全身蛋白质组提供了新的见解,并鉴定出具有诊断潜力的新型蛋白质生物标志物。