Allen Margaret E, Beck Ryan T, Zwagerman Nathan T, Coss Dylan, Fisco Amy, Ioachimescu Adriana G
Medical College of Wisconsin, Milwaukee, WI 53226 USA.
Department of Radiology, Medical College of Wisconsin, Milwaukee, WI 53226 USA.
JCEM Case Rep. 2024 Oct 16;2(10):luae182. doi: 10.1210/jcemcr/luae182. eCollection 2024 Oct.
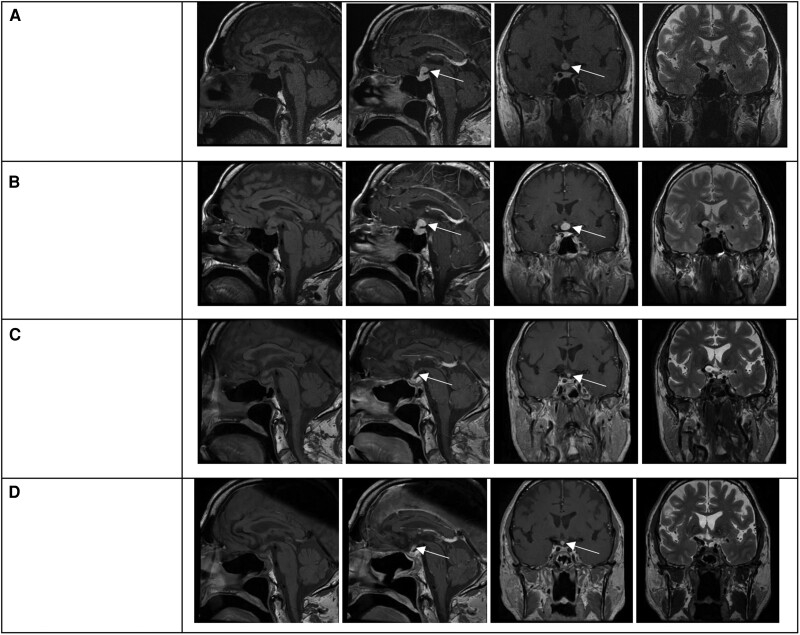
A 72-year-old man presented with several months of weakness, poor appetite, and depressed moods. Laboratory tests indicated central hypocortisolism, hypothyroidism and hypogonadism, and mild hyperprolactinemia. Imaging indicated a homogenously enhancing solid suprasellar mass inseparable from the hypothalamus and contiguous with a thickened proximal infundibulum. Neuro-ophthalmological evaluation was normal. Symptoms improved with hydrocortisone, levothyroxine, and testosterone replacement. After 6 months, transsphenoidal biopsy was performed due to mass enlargement and revealed fibrosis, lymphoplasmacytic infiltration, and CD138 and IgG4 staining. The levels of serum IgG4, complement, inflammatory markers, protein electrophoresis, amylase, and lipase and imaging of the chest, abdomen, and thyroid were unremarkable. After 1 month of prednisone therapy (starting dose 40 mg/day), the mass significantly involuted and remained stable afterward. Prednisone was gradually tapered to 5 mg daily over 10 weeks. During 22 months of follow-up, no systemic IgG4 disease was detected. Glucocorticoid, thyroid, and testosterone replacement was continued. This case of isolated IgG4-related hypophysitis illustrates the variable presentation that may not entail vasopressin deficiency or clinical mass effect. This entity should be considered in the differential diagnosis of suprasellar masses even in the absence of IgG4 systemic disease or characteristic serology. Management entails multidisciplinary collaboration and long-term follow-up.
一名72岁男性,出现数月的乏力、食欲减退和情绪低落。实验室检查提示中枢性皮质醇减少、甲状腺功能减退和性腺功能减退,以及轻度高泌乳素血症。影像学检查显示鞍上有一个均匀强化的实性肿块,与下丘脑无法区分,并与增厚的漏斗部近端相连。神经眼科评估正常。氢化可的松、左甲状腺素和睾酮替代治疗后症状改善。6个月后,由于肿块增大进行了经蝶窦活检,结果显示纤维化、淋巴细胞浆细胞浸润,以及CD138和IgG4染色阳性。血清IgG4、补体、炎症标志物、蛋白电泳、淀粉酶和脂肪酶水平以及胸部、腹部和甲状腺的影像学检查均无异常。泼尼松治疗1个月(起始剂量40mg/天)后,肿块明显缩小,之后保持稳定。泼尼松在10周内逐渐减量至每日5mg。在22个月的随访中,未检测到系统性IgG4疾病。继续进行糖皮质激素、甲状腺和睾酮替代治疗。这例孤立性IgG4相关性垂体炎说明了其临床表现的多样性,可能不伴有血管加压素缺乏或临床占位效应。即使在没有IgG4系统性疾病或特征性血清学表现的情况下,在鞍上肿块的鉴别诊断中也应考虑到这一疾病。治疗需要多学科协作和长期随访。