Service de Médecine Intensive-Réanimation, Hôpital de La Croix Rousse, Hospices Civils de Lyon, Lyon, France.
Univ Lyon, Université Claude Bernard Lyon 1, INSA-Lyon, CNRS, INSERM, CREATIS UMR 5220, U1294, Villeurbanne, France.
Intensive Care Med. 2024 Dec;50(12):2061-2072. doi: 10.1007/s00134-024-07676-1. Epub 2024 Oct 17.
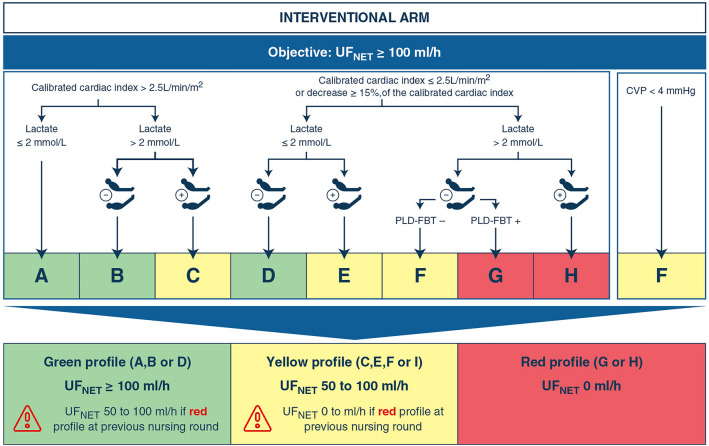
Net ultrafiltration (UF) during continuous renal replacement therapy (CRRT) can control fluid balance (FB), but is usually 0 ml·h in patients with vasopressors due to the risk of hemodynamic instability associated with CRRT (HIRRT). We evaluated a UF strategy adjusted by functional hemodynamics to control the FB of patients with vasopressors, compared to the standard of care.
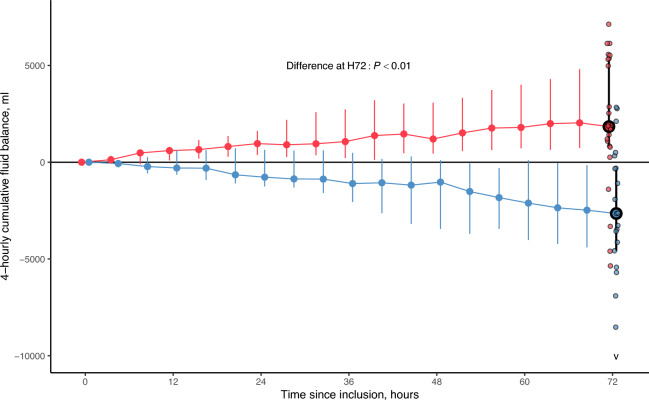
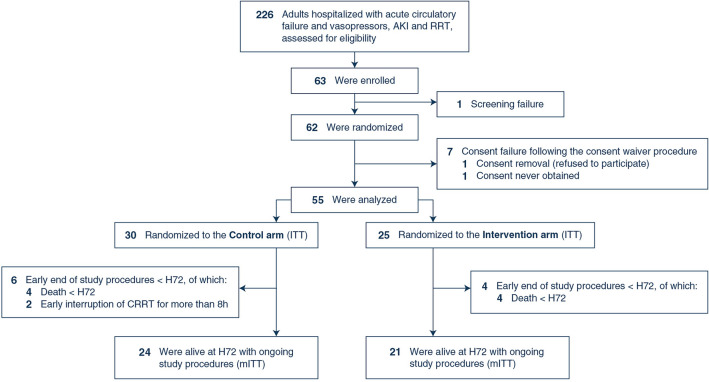
In this randomized, controlled, open-label, parallel-group, multicenter, proof-of-concept trial, adults receiving vasopressors, CRRT since ≤ 24 h and cardiac output monitoring were randomized (ratio 1:1) to receive during 72 h a UF ≥ 100 ml·h, adjusted using a functional hemodynamic protocol (intervention), or a UF ≤ 25 ml·h (control). The primary outcome was the cumulative FB at 72 h and was analyzed in patients alive at 72 h and in whom monitoring and CRRT were continuously provided (modified intention-to-treat population [mITT]). Secondary outcomes were analyzed in the intention-to-treat (ITT) population.
Between June 2021 and April 2023, 55 patients (age 69 [interquartile range, IQR: 62; 74], 35% female, Sequential Organ Failure Assessment (SOFA) 13 [11; 15]) were randomized (25 interventions, 30 controls). In the mITT population, (21 interventions, 24 controls), the 72 h FB was -2650 [-4574; -309] ml in the intervention arm, and 1841 [821; 5327] ml in controls (difference: 4942 [95% confidence interval: 2736-6902] ml, P < 0.01). Hemodynamics, oxygenation and the number of HIRRT at 72 h, and day-90 mortality did not statistically differ between arms.
In patients with vasopressors, a UF fluid removal strategy secured by a hemodynamic protocol allowed active fluid balance control, compared to the standard of care.
连续性肾脏替代治疗(CRRT)期间的净超滤(UF)可以控制液体平衡(FB),但由于与 CRRT 相关的血流动力学不稳定(HIRRT)的风险,对于接受血管加压药的患者通常为 0 ml·h。我们评估了一种通过功能性血流动力学调整的 UF 策略来控制接受血管加压药的患者的 FB,与标准护理相比。
在这项随机、对照、开放标签、平行组、多中心、概念验证试验中,接受血管加压药、CRRT 时间≤24 小时和心输出量监测的成年人被随机分为 72 小时接受 UF≥100 ml·h(干预组)或 UF≤25 ml·h(对照组),使用功能性血流动力学方案调整 UF。主要结局是 72 小时时的累积 FB,并且在 72 小时时存活的患者和持续提供监测和 CRRT 的患者中进行分析(修改意向治疗人群[mITT])。次要结局在意向治疗(ITT)人群中进行分析。
2021 年 6 月至 2023 年 4 月,共纳入 55 例患者(年龄 69 [四分位距:62;74],35%女性,序贯器官衰竭评估[SOFA]13 [11;15]),随机分为 25 例干预组和 30 例对照组。在 mITT 人群中(21 例干预组,24 例对照组),干预组 72 小时 FB 为-2650[-4574;-309]ml,对照组为 1841[821;5327]ml(差异:4942[95%置信区间:2736-6902]ml,P<0.01)。72 小时时的血流动力学、氧合和 HIRRT 的数量以及 90 天死亡率在两组之间没有统计学差异。
在接受血管加压药的患者中,通过血流动力学方案保证的 UF 液体清除策略与标准护理相比,可实现积极的液体平衡控制。